
Apophyseal Metaphyseal combination injury to Olecranon in a healthy Adolescent – A rare injury and review of literature
Vol 1 | Issue 1 | July-Sep 2015 | page:51-53 | Ganesh Singh Dharmshaktu, Anshuman Vijay Roy.
Authors : Ganesh Singh Dharmshaktu[1], Anshuman Vijay Roy[2].
[1] Department of Orthopaedics, Government Medical College, Haldwani , Uttarakhand.
[2] Department of Orthopaedics, Krishna Hospital and Research Centre, Haldwani , Uttarakhand.
Address of Correspondence
Dr. Ganesh Singh Dharmshaktu , Department of orthopaedics , Government Medical College , Haldwani ( Uttarakhand ) . PIN -263139. Email: drganeshortho@gmail.com
Abstract
Background: Apophyseal injuries of olecranon have limited number of case reports and series owing to its rarity. Pure apophyseal avulsions are very rare and so are apophyseal metaphyseal combination injuries. No guidelines exist for the uniformity of the treatment and various modalities have been tried in sporadic reports. A keen clinical observation is required to suspect the possibility of these injuries followed by good imaging confirmation. Concordance of associated disorders like osteogenesis imperfecta with such injuries underlines the importance of ruling out this clinical entity in such cases.
Keywords: Fracture, Apophysis, Olecranon, Injury. Tension band wiring.
Introduction
Upper extremity is common site of bony injuries in children with reported incidence of 65% to 75% in the literature. 7% to 9% of these injuries are elbow injuries.[1] Apophysis is a term usually applied to an epiphysis that is subjected to traction by muscle insertion and its physiological pull.[2] The injury to the region if displaced can cause serious morbidity and functional limitation and thus warrants appropriate treatment. Non operative management is limited to only undisplaced injuries while injuries with more than 3-5 mm. of displacement warrants open reduction followed by fixation with varying methods. Open reduction and compressive fixation has widely been tried successfully with various implants like screws, tension band wiring or resorbable sutures. There has not been significant growth related problem with compression forces as a result of internal fixation.[2]
Case Report
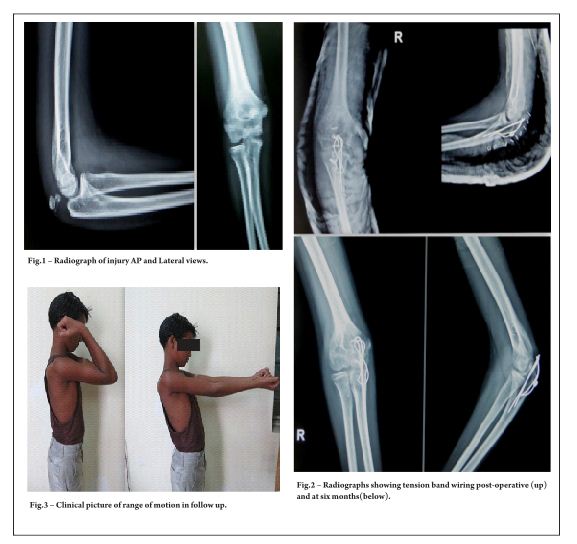
A 12 year old boy was presented to us with history of injury to his right elbow following fall from height two days back. He was taken to a local practitioner before coming to us with a make do splint of wooden sticks. There was swelling, pain and difficulty in using the affected limb. There was tenderness present and swelling more over the posterior aspect but no raised temperature and intact distal neurovascular status. There was no appreciable crepitus or frank abnormal mobility present and a proper elbow examination including range of motion status was limited by swelling and pain. The radiograph of the affected elbow showed an apophyseal-metaphyseal combination injury with displacement. The olecranon apophysis with a rim of metaphysis was avulsed. There was no associated injury present. There was neither any history of frequent or multiple bony injuries in the past related or remote to present condition nor presence of blue sclera or abnormal dentition. The parents of the boy were explained and advised operative intervention of the injury. Following an informed consent of parents in view of patient being minor and under aseptic precautions open reduction and internal fixation was planned and carried out.
Result
The open reduction and internal fixation was performed and secured with tension band wiring (TBW). The posterior approach was used to access the injury site, The avulsed part was provisionally reduced and held together with pointed clamps while TBW was carried out in standard manner using two parallel Kirschner’s wires and a wire loop in figure of eight fashion. The operation went uneventful and so was peri-operative period. The stitches were removed on tenth day and patient was advised supervised physiotherapy after two weeks. The follow up initially at three, six twelve weeks and then after three and six months were uncomplicated and the range of motion improved all this while. The final follow up at six months showed normal range of motion as compared to contra-lateral side. There was no problem with hardware in the follow up and those were removed subsequently after months.
Discussion
The type 3 injuries related to olecranon apophyses are complete fractures with type 3 (a) as pure avulsions and type 3(b) as apophyseal-metaphyseal combination injuries.[2] Type 3(b) injuries are commoner in older children while type 3(a) usually involves younger children. This pattern of injury has been likened to Salter-Harris type 2 injury.[3] Apophyseal injuries of olecranon are uncommon with limited reported incidents.[4] Most of these injuries have been associated with patients of osteogenesis imperfecta.[5] Osteognesis imperfecta cases ( like tarda form) show higher incidences for this injury.[6] Apart from the fact that olecranon apophyses fractures are reported in relation with 50% cases of osteogenesis imperfecta, there have been reportedly higher rates of complication such as refracture in them.[7] It has been advised that hardwares should be maintained even after union in cases of osteogenesis imperfect due to this risk.[5,7] The elbow has rich vascularity with extraosseus network as well as intraosseus one.[8,9] The undisplaced fractures are amenable to conservative treatment with plaster of paris slab or cast and fracture unite well if length, angulation and rotation is properly taken care of. The displaced fractures has been managed with tension band wiring in most instances with fair to excellent results.[3,7,10] Some authors have used trans- osseous suture fixation for the fractures with good results.[11] Use of absorbable wires as supplemental fixation have also been reported.[12] As most of these injuries occur in children near skeletal maturity, no significant growth related problem is seen as compressive fixation across physes. The presented case is an uncommon variant of apophyseal olecranon injury in a normal child managed satisfactorily with appropriate techniques.
References
1. Landin LA, Danielsson LG. Elbow fractures in children: an epidemiological analysis of 589 cases. Acta Orthop Scand 1986; 57:309.
2. Erickson M, Frick S. Fractures of the proximal radius and ulna.In Beaty JH, Kasser JR. editors. Rockwood and Wilkins Fractures in children 7th ed. Philadelphia: Lippincott Williams and Wilkins;2010: 427-431.
3. Granthan SA, Kiernan HA. Displaced olecranon fractures in children. J Trauma 1975;15197-204.
4. Carney JR, Fox D, Mazurek MT. Displaced apophyseal olecranon fracture in a healthy child. Mil Med. 2007;172(12):1225-7.
5. Zionts LE, Moon CN. Olecranon apophysis fractures in children with osteogenesis imperfecta revisited. J Pediatr Orthop.2002; 22(6):745-50.
6. Di Cesare PE, Sew-Hoy A, Krom W. Bilateral isolated olecranon fractures in an infant as presentation of osteogenesis imperfect. Orthopedics 1992; 15:741-743.
7. Gwynne-Jones DP. Displaced olecranon apophyseal fractures in children with osteogenesis imperfecta. J Pediatr Orthop. 2005; 25(2):154-7.
8. Wilson PD. Fractures and dislocations in the region of elbow. Surg Gynecol Obstet 1933;56:335-359.
9. Haraldsson S. The intraosseous vasculature of the distal end of humerus with special reference to capitellum. Acta Orthop Scand 1957;27:81-93.
10. Poland J. A Practical Treatise on Traumatic Separation of the Epiphyses. London; Smith, Elder & Co, 1898.
11. Rath NK, Carpenter EC, Thomas DP. Traumatic pediatric olecranon injury: a report of suture fixation and review of the literature. Pediatric emergency care 2011; 27(12):1167-9.
12. Gortzak Y,Mercado E, Atar D, et al. Pediatric olecranon fractures: open reduction and internal fixation with removable Kirschner wires and absorbable sutures. J Pediatr Orthop 2006;26:39-42
.
| How to Cite this Article: Dharmshaktu GS, Roy AV. Apophyseal- metaphyseal combination injury to olecranon in a healthy adolescent – A rare injury and review of literature. International Journal of Paediatric Orthopaedics July-Sep 2015;1(1):51-53. |

