
Clinical and Radiological Outcome following Kim’s Step cut Translation Osteotomy for Cubitus Varus and Valgus in Children
Volume 2 | Issue 2 | May-Aug 2016 | Page 34-37|Dhurvas Ramlal Ramprasath, Vasudevan Thirunarayanan, Murugan Shanmuga Sundaram
Authors :Dhurvas Ramlal Ramprasath [1], Vasudevan Thirunarayanan [1], Murugan Shanmuga Sundaram [2]
[1] Senior Assistant Professor, Department of Orthopaedic Surgery, Government Royapettah Hospital,Westcott road,Royapettah,Chennai,India-600014.
[2] Junior Resident, Department of Orthopaedic Surgery, Government Royapettah Hospital, Chennai, India- 600014.
Address of Correspondence
Dr Ramprasath D.R.,
12/23, Murugappa street, Purasawakkam, Chennai, India. PIN- 600007.
Email ID: dhurvasramprasath@gmail.com
Abstract
Several osteotomies are available to correct cubitus varus and valgus deformities in children. The purpose of this study was to evaluate clinical and radiological outcome following Kim’s step cut translation osteotomy for such deformities.
Materials and Methods: We have instituted Kim’s step cut translational osteotomy in seven children having deformities of elbow (cubitus varus – 4 and cubitus valgus – 3). Patients were followed up for a period of 8 to 14 months during the period of August 2014 to October 2015. Clinically and radiologically, preoperative and postoperative Humerus-Elbow-Wrist angle, Range of motion of elbow, Lateral/Medial Prominence Index and neurological examination for ulnar nerve were determined. Results were evaluated according to modified Oppenheim et al criteria.
Results: The mean postoperative Humerus-Elbow-Wrist angle in patients with cubitus varus was 8.5±2.06 0 (range, 50 to 100). The mean improvement in Lateral Prominence Index was 7.4 ±1.28% (from –13.15% to -5.75% ). In cubitus valgus patients, mean
postoperative Humerus-Elbow-Wrist angle was 12.33±3.510(range, 80 to 150) . The mean improvement in MPI was 8.7±0.83% (from -15.5% to -6.8% ) . In all patients range of motion was comparable with normal side elbow. Bone union was achieved in all patients. According to Oppenheim’s criteria, six patients had excellent results and one patient had good result. .None of them had any complications.
Conclusion: Even though multiple procedures are available for correcting deformities of elbow, Kim’s step cut translational osteotomy provides good correction angle, lesser prominence of the condyle, better stability and three dimensional correction.
Key Words: Cubitus varus, Cubitus valgus, Kim’s osteotomy, Lateral/ Medial prominence Index.
Introduction
Cubitus varus and valgus deformities are complications of elbow fractures in children[1]. Cubitus varus has multiple components that include varus malalignment, hyperextension and internal malrotation[2,3]. The most important indication for osteotomy is to achieve a good cosmesis[2,4]. Many surgical techniques have been described to correct these deformities including closing wedge, opening wedge, dome and step cut osteotomies[5-12]. The closing wedge osteotomy has a tendency to produce prominent condyles after correction,often compromising the cosmetic outcome[2,13-16]. The inclusion of translation in the osteotomy improves cosmetic appearance by minimizing the persistent prominence of the medial or lateral condyle. This can be achieved by Kim’s osteotomy. The aim of our study was to evaluate clinically and radiologically, the preoperative and postoperative Humerus-Elbow-Wrist(HEW) angle, Lateral/Medial Prominence Index(LPI/MPI), Range of Motion(ROM), in children undergoing Kim’s step cut translation osteotomy for cubitus varus and valgus.
Materials and Methods
This is a retrospective study, from August 2014 to October 2015, involving seven paediatric patients in the age group 8 – 14 years with male:female ratio of 4:3. Those with cubitus varus deformity had sustained supracondylar humerus fracture and those with valgus deformity had fracture lateral condyle. All the patients had undergone native treatment immediately after injury, and presented to our department after a period of 14 months to 34 months after injury.
We have instituted step cut translational osteotomy of Hui Taek Kim [1] in all the seven patients. Preoperatively, radiological and clinical planning includes measurement of HEW angle, lateral/medial prominence index (using the method described by Wong et al [2,16]),range of motion of elbow, neurological examination for ulnar nerve and internal rotation malalignment (using the method described by Yamamoto[17,18]). Same radiological and clinical parameters were evaluated postoperatively.
HEW angle was measured by drawing two lines, one line along the anatomical axis of humerus ,and another line joining midpoints of two transverse lines(one proximal and one distal) across the forearm that connected the medial cortex of ulna and lateral cortex of radius (Fig-1). The Lateral/Medial Prominence Index was measured by using the formula shown in (Fig-2).
We determined the Correction Angle (CA) for patients with cubitus varus by adding varus HEW angle with normal side HEW angle, and for patients with cubitus valgus by subtracting normal side HEW angle from affected side valgus HEW angle. A template using X-ray film, was prepared preoperatively, to mark the site and size of osteotomy, using following technique(Fig-3).
The outline of the bone was drawn on a trace paper. A horizontal line was drawn perpendicular to anatomical axis of humerus at a level 0.5 to 1 cm proximal to the olecranon fossa. Now the trace paper was cut along the horizontal line and the distal fragment was rotated laterally and translated medially(in case of cubitus varus) so as to achieve HEW angle of normal side. Vice versa was done for cubitus valgus deformity. An inverted V was marked on the trace paper. We then cut out the triangular overlapping area from the paper and prepared X-ray film of same size and shape. This triangular X-ray film was sterilised for
use during osteotomy.
 Angle") Figure 1: Humerus-Elbow-Wrist (HEW) Angle |
LPI (%)=(AB-BC)/AC×100,LPI (%)=(AB-BC)/AC×100") Figure 2: Lateral/Medial Prominence Index % (LPI/MPI) LPI (%)=(AB-BC)/AC×100 LPI (%)=(AB-BC)/AC×100 |
 Figure 3: Preop Templating |
Method of Osteotomy
With the patient in lateral decubitus position,through posterior approach ,ulnar nerve was isolated and protected. The triceps aponeurosis was split. The triangular X-ray template (turned face downward because of posterior approach) was placed over the bone 1cm proximal to olecranon fossa and necessary osteotomy was done to remove an identical piece of bone. The distal fragment was rotated laterally for cubitus varus(and medially for cubitus valgus) and inserted into the inverted V shaped defect. The deformity correction was assessed clinically and then the fixation was done with distal radius T-Plate and 3.5mm cortical
screws. The ulnar nerve was transposed anteriorly in patients who had tardy ulnar nerve palsy due to cubitus valgus deformity.
Patient was immobilised in long arm slab for 2 weeks following which active and assisted mobilisation was done intermittently retaining the splint until radiological union was achieved.
Results
The HEW angle, LPI/MPI, ROM were measured and analysed (Table -1).
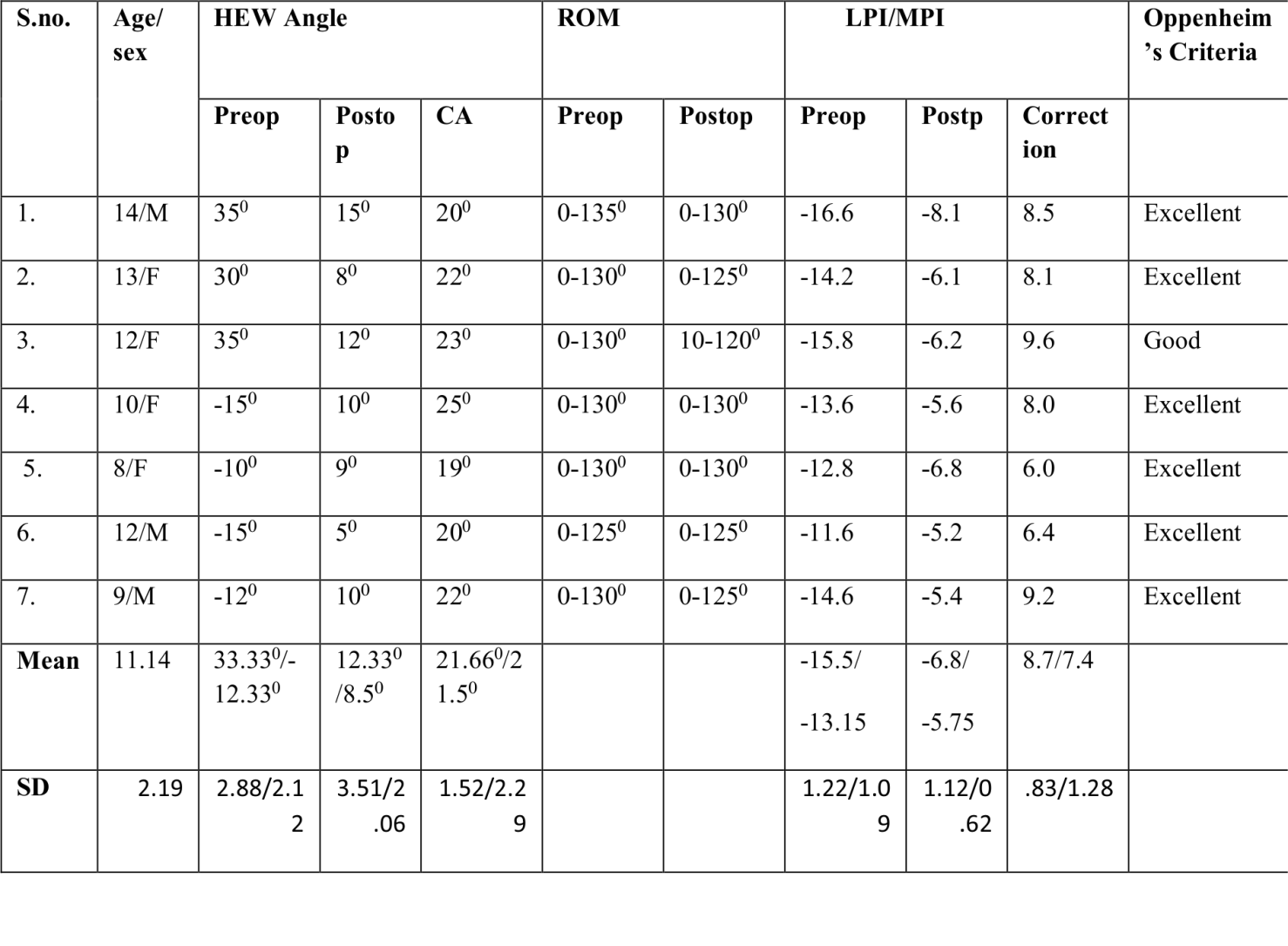
Table-1: Preoperative and Postoperative Measurements.
HEW- Humerus-Elbow-Wrist angle, LPI /MPI – Lateral/Medial Prominence Index, CA- Correction Angle
In cubitus varus patients, mean postoperative HEW angle was 8.50(range, 50to 100),with mean correction of 21.50(range,190 to 250). The mean improvement in LPI was 7.4% (from -13.15% to -5.75% ) .In cubitus valgus patients(Fig-5), mean postoperative HEW angle was 12.330(range, 80 to 150),with mean correction of 21.660(range,200 to 230). The mean improvement in MPI was 8.7% (from -15.5% to -6.8% ).In all patients, range of motion was comparable with normal side elbow (Table 1). Pronation and supination movements were normal in all our cases. Bone union was achieved in all patients.
 Figure 4: Osteotomy and Fixation |
") Figure 5: X-ray(Preop and Postop) |
According to Oppenheim’s criteria [7], excellent result (Fig-6) was achieved in 6 patients and good result in one patient, and no patient had poor result.
")
Figure 6: Lateral/Medial Prominence Index % (LPI/MPI)
Discussion
In patients with cubitus varus/valgus, the following problems need to be addressed deformity correction in coronal plane(valgus/varus), sagittal plane(fixed flexion/hyperextension),horizontal plane(internal/external rotation deformity); ulnar nerve palsy, if any.
The deformity is better corrected during childhood. Correction, particularly in cubitus varus, in adult is challenging due to mature skeleton, inherent instability at osteotomy site, risk of delayed union/non union, implant failure, infection, stiffness and neurovascular complications [19]. A rough estimate will be around a year after original injury. Again patient demands, growth potential and status of physis should be taken into account while planning surgery[20].
Major types of osteotomies are – simple closing wedge [17,21,22],step cut translation [1,17,23], dome rotational osteotomy[13,14,17,24] and spike translation osteotomy[17]. Many of these osteotomies have got their own disadvantages, like lateral scar, medial and lateral condylar prominence and difficulty in correcting rotational deformities( due to contractures)[1,24,25,26].
Various method of fixation include use of K-wires, screws, plates and external fixators (Ilizarov technique) [5,13,25,27-29]. We have used Kim’s method of step cut translation Osteotomy, and fixed with distal radius T-plate.
This method has got multiple advantages. Adequate Correction Angle (CA) is achieved by moving the apex more medially (in cubitus varus) or laterally (in cubitus valgus). The stability of fixation is enhanced because the distal fragment is inserted into the inverted V shaped proximal fragment and fixation was done with plates. The prominence of condyles (lateral condyle in cubitus varus and medial condyle in cubitus valgus) is less with Kim’s osteotomy (when compared to other methods ) because distal fragment is translated. With Kim’s osteotomy, three dimensional correction is possible. The correction of internal rotation is recommended when the difference in rotational alignment in both sides is greater than 100 [1,17,18]. In our study ,we did not encounter patient with hyperextension, or internal rotation more than 100, when compared to normal side. Hence we have not attempted correction in sagittal/horizontal planes.
The limitations of our study is smaller sample size and follow up of only 14 months duration.
Conclusion
This simple step cut translation osteotomy(Kim’s) results in good cosmetic deformity correction,very firm fixation,earlier elbow movement and also avoids problems of condylar prominence and non union. Deformities in sagittal/horizontal plane can also be corrected.
References
1. Hui taek kim, md, Jung sub lee, md, and Chong il yoo, md. Management of cubitus varus and valgus. The journal of bone & joint surgery.Volume 87-a , number 4, april 2005.
2. K. Bali , P. Sudesh, V. Krishnan, A. Sharma, S.R.R. Manoharan, A.k. Mootha. Modified step-cut osteotomy for post-traumatic cubitus varus: our experience with 14 children. Orthopaedics & traumatology: surgery & research (2011) 97, 741-749.
3. Takagi T, Takayama S, Nakamura T, Horiuchi Y, Toyama Y,Ikegami H. Supracondylar osteotomy of the humerus to correct cubitus varus: Do both internal rotation and extension deformities need to be corrected? J bone joint surg am 2010;92(7):1619-26.
4. Pankaj A, Dua A, Malhotra A, Bhan S. Dome osteotomy for posttraumatic Cubitus varus a surgical technique to avoid lateral condylar prominence. J pediatr orthop 2006;26(1):61-6.
5.Y.H. Yun,S.J. Shin,J.G. Moon. Reverse v osteotomy of the distal humerus For the correction of cubitus varus. J bone & joint surg [br].2007;89-b:527-31.
6.Derosa GP, Graziano GP. A new osteotomy for cubitus varus. Clin orthop 1988;236:160-5.
7. Kanaujia RR, Ikuta Y, Muneshige H, Higaki T, Shimogaki K. Dome osteotomy for cubitus varus in children. Acta orthop scand 1988;59:314-17.
8. Kim HS, Jahng JS, Han DY, et al. Modified step-cut osteotomy of the humerus. J Pediatr orthop b 1988;7:162-6.
9. Koch PP, Exner GU. Supracondylar medial open wedge osteotomy with external fixation For cubitus varus deformity. J pediatr orthop b 2003;12:116-22.
10. Laupattarakasem W, Mahaisavariya B, Kowsuwon W, Saengnipanthkul S. Pentalateral osteotomy for cubitus varus: clinical experiences of a new technique. J Bone joint surg [br] 1989;71-b:667-70.
11. Oppenheim WL, Clader TJ, Smith C, Bayer M. Supracondylar humeral osteotomy For traumatic childhood cubitus varus deformity. Clin orthop 1984;188:34-9.
12. Uchida Y, Ogata K, Sugioka Y. A new three-dimensional osteotomy for cubitus Varus deformity after supracondylar fracture of the humerus in children. J pediatr Orthop 1991;11:327-31.
13. Bellemore MC, Barrett IR, Middleton RW, Scougall JS, Whiteway DW. Supracondylar osteotomy of the humerus with correction of cubitus varus. J bone joint surg br 1984;66(4):566-72.
14. Matsushita t, Nagano a. Arc osteotomy of the humerus to correct cubitus varus. Clin orthop relat res 1997;336:111-5.
15. Tien YC, Chih HW, Lin GT, Lin SY. Dome corrective osteotomy for cubitus varus deformity. Clin orthop relat res 2000;380:158-66.
16.Wong HK, Lee EH, Balasubramaniam P.The lateral condylar prominence. A complication of supracondylar osteotomy for cubitus varus. J bone joint surg br 1990;72:859-61.
17. Ali Moradi MD, Ehsan Vahedi MD,Mohammad H.Ebrahimzadeh MD. Spike Translation: A New Modification in Step-cut Osteotomy for Cubitus Varus Deformity. Clin Orthop Relat Res (2013) 471:1564–1571.
18. Yamamoto I, Ishii S, Usui M, Ogino T, Kaneda K. Cubitus varus deformity following supracondylar fracture of the humerus: a method for measuring rotational deformity. Clin Orthop Relat Res. 1985;201:179–185.
19. S Pandey, A Shrestha, AP Regmi, A Prajapati, S Dhakal and G Neupane. Cubitus varus in young adults correction with lateral closing wedge osteotomy and screw, k-wire and ss-wire fixation.Journal of Chitwan Medical College; 2012, 1(2); 60-62.
20. Sandeep patwardhan , Ashok k shyam. Cubitus varus deformity – rationale of treatment and methods. International journal of paediatric orthopaedics | volume 1 | issue 1 | july-sep 2015 | page 26-29.
21. Graham B, Tredwell SJ, Beauchamp RD, Bell HM. Supracondylar osteotomy of the humerus for correction of cubitus varus. J Pediatr Orthop. 1990;10:228–231.
22. Voss FR, Kasser JR, Trepman E, Simmons E Jr, Hall JE. Uniplanar supracondylar humeral osteotomy with preset Kirschner wires for posttraumatic cubitus varus. J Pediatr Orthop. 1994;14:471–478.
23. Davids JR,Lamoreaux DC, Brooker RC,Tanner SL, Westberry DE.Translation step-cut osteotomy for the treatment of posttraumatic cubitus varus.J Pediatr Orthop. 2011;31:353-365
24. Labelle H, Bunnell WP, Duhaime M, Poitras B. Cubitus varus deformity following supracondylar fractures of the humerus in children. J Pediatr Orthop. 1982;2:539–546.
25. French PR. Varus deformity of the elbow following supracondylar fractures of the humerus in children. Lancet. 1959;2:439-41.
26. King D, Secor C. Bow elbow (cubitus varus). J Bone Joint Surg Am. 1951; 33:572-6.
27. Carlson CS Jr, Rosman MA. Cubitus varus: a new and simple technique for correction. J Pediatr Orthop 1982;2:199-201.
28. Levine MJ. Horn BD, Pizzutillo PD. Treatment of posttraumatic cubitus varus in pediatric population with humeral osteotomy and external fixation. J Pediatr Orthop 1996;16:597-601.
29. Karatosun V, Alekberov C, Alici E, Ardic CO, Aksu G. Treatment of cubitus varus using the Ilizarov technique of distraction osteogenesis. J Bone Joint Surg [Br]2000;82-B:1030-3.
| How to Cite this Article: Ramprasath DR, Thirunarayanan V, Sundaram MS. Clinical and radiological outcome following Kim’s Step Cut Translation Osteotomy for Cubitus Varus and Valgus in Children International Journal of Paediatric Orthopaedics May-Aug 2016;2(2):34-37. |
 Dr Dhurvas Ramlal Ramprasath |
 Dr. Vasudevan Thirunarayanan |
 Dr. Murugan Shanmuga Sundaram |

