Complications of Surgical Management of Radial Club Hand
Volume 2 | Issue 3 | Sep-Dec 2016 | Page 24-27| Ratna Maheshwari, Rujuta Mehta, Ashok Johari
Authors : Ratna Maheshwari [1], Rujuta Mehta [2], Ashok Johari [3]
[1] Consultant, Pediatric Orthopedics, Enable International Centre for Pediatric Musculoskeletal Care
[2] Head of Dept. Paediatric Orthopedics B J Wadia Hospital For Children.
[3] Head, Pediatric Orthopedics, Enable International Centre for Pediatric Musculoskeletal Care.
Address of Correspondence
Dr Ratna Maheshwari
Enable International Centre for Pediatric Musculoskeletal Care
Email: drratnajohari@gmail.com
Abstract
Radial club hand is a congenital deformity of the upper extremity which can present with a spectrum of hand and forearm anomalies ranging from mild radial hypoplasia to complete absence of the radius. The surgical treatment of radial club hand historically has attempted to create a centralized wrist, maintain wrist motion and improve hand function by placing the hand in a more outstretched position.Treatment for these patients has focused on the technique of centralization, in addition to ulnocarpal arthrodesis, ulna and radial lengthening, and microvascular toe transfer. In this paper we review the complications of various surgical interventions described so far for the treatment of this condition.
Keywords: Centralization, recurrence, physeal arrest.
Introduction
There are several treatment options for radial deficiency of the forearm, including nonsurgical management; centralization, radialization, or ulnarization; ulnocarpal arthrodesis; soft tissue procedures including distraction; ulnar lengthening; and vascularized second metatarsophalangeal joint transfer. The most common procedure performed currently is soft tissue distraction followed by a wrist realignment procedure such as a centralization, radialization, or ulnarization. While one-stage procedures subject the patient to a single operation, they are associated with the possible need for carpal resections, ulnar shortening, and sacrifice of the distal ulnar growth plate, stretch injury to the radial neurovascular structures, excessive swelling of the hand, and wound complications [1,2,3,4,5,6]
Centralization/radialization/ulnarization
This technique involves moving the carpus to a central position on the ulna as a means of obtaining correction of radial deviation and wrist subluxation. Unfortunately, this technique has been associated with a high rate of recurrent radial deviation, physeal injury and wrist stiffness [7,8]
Lamb et al [9] reported a recurrence of radial wrist deviation in 7 out of 15 patients.
Damore and colleagues reviewed 19 cases of recurrence after a centralization procedure. The surgery had corrected the radial deviation from a mean of 83 to 25.However at final follow- up (6.5 years), the deviation was back to an average of 63 [10].
Heikel [11] demonstrated in 1959 that the ulna in children with radial club hand may grow between one half to three quarters the length of the unaffected ulna. Centralization procedures, with concomitant ulnar osteotomy and transphyseal pins can all result in potential distal ulnar physeal injury resulting in further shortening of the forearm unit.
In their long-term outcome study, Goldfarb et al [12] noted total ulnar growth to average 12 cm in comparison to 15.4 cm in Vilkki’s series [13] of vasularised metatarsophalangeal joint transfer . While 3 cm may seem clinically insignificant, this must be taken in the context of a longer ulna in addition to a wrist that is in a more balanced position when compared to standard centralization procedures.
K-wire stabilisation is not free of complications: wire migration or breakage, skin ulcer, and changes may follow growth. Despite such repeated revision, correction loss is acceptable and the fixation finally stabilizes over growth. If K-wire tension appears excessive, distraction can be slowed down so as to allow the skin and capsule-ligamentous structures to relax progressively [14].
Ulnocarpal arthrodesis
This procedure is generally reserved for recurrence of deformity after centralization. The generally accepted indications for this procedure is radial angulation greater than 450, inability to actively extend the wrist to within 250 of neutral. Pike et al [15] described 12 patients with average age of 12.6 years treated with ulnocarpal arthrodesis for recurrence of deformity after centralization, that was performed at an average age of 2.4 years. The average time to union for 11 of the 12 patients was 4 months. Union was ultimately achieved in the 12th patient after a revision arthrodesis with a plate that was necessary because the initial arthrodesis hardware (K-wires) was removed early owing to concern about infection.
Ulnar lengthening
Farr and colleagues [16] reported on 8 cases in 6 patients and noted that initial postsurgical gains of radial deviation were not maintained. Radial deviation averaged 250 preoperatively and recurred to 230 at an average 4-year follow-up. Two major complications occurred, including an ulna fracture after frame removal and insufficient regenerate during lengthening.
Peterson and colleagues [17] described 9 children who underwent 13 lengthenings after previous centralization procedures. The average gain in length was 4.4 cm. All patients had at least 1 pin site infection that was treated with antibiotics. Furthermore 4 patients had additional procedures, including internal fixation and bone grafting for delayed union in 3 patients and wrist arthrodesis for recurrence in 1 patient.
Yoshida and colleagues [18] investigated the growth of the ulna after repeated lengthenings. After the initial lengthening, the average length improved from 57% to 89% of the normal side, but then regressed to 70%, whereas after the second lengthening the average length was 102% but regressed to 83%. Bone growth was found to be markedly decreased after the second lengthening. Therefore, if multiple lengthenings are performed, the second one should be performed after skeletal maturity.
Although successful in producing multi-planar deformity correction and an approximately 50% increase in ulnar length, the Ilizarov technique brings with it a steep clinician learning curve. Device application, cumbersome hardware, lengthy total treatment time, and relatively high risk of complications may prove problematic and has effectively limited the use of the device to adolescents and older children.

Radial lengthening
Matsuno and colleagues [19] described 4 cases of Bayne and Klug type II and III radial longitudinal deficiency treated with radial lengthening and simultaneous soft tissue distraction. Three of 4 patients required several lengthenings to correct the recurring discrepancy between the radius and ulna. Only 2 of the 4 patients had acceptable function and appearance after the multiple procedures. In 1 patient, lengthening was abandoned owing to severe bone absorption at the distal end of the radius. One patient died of cardiac disease after a lengthening.
Microvascular second toe transfer:
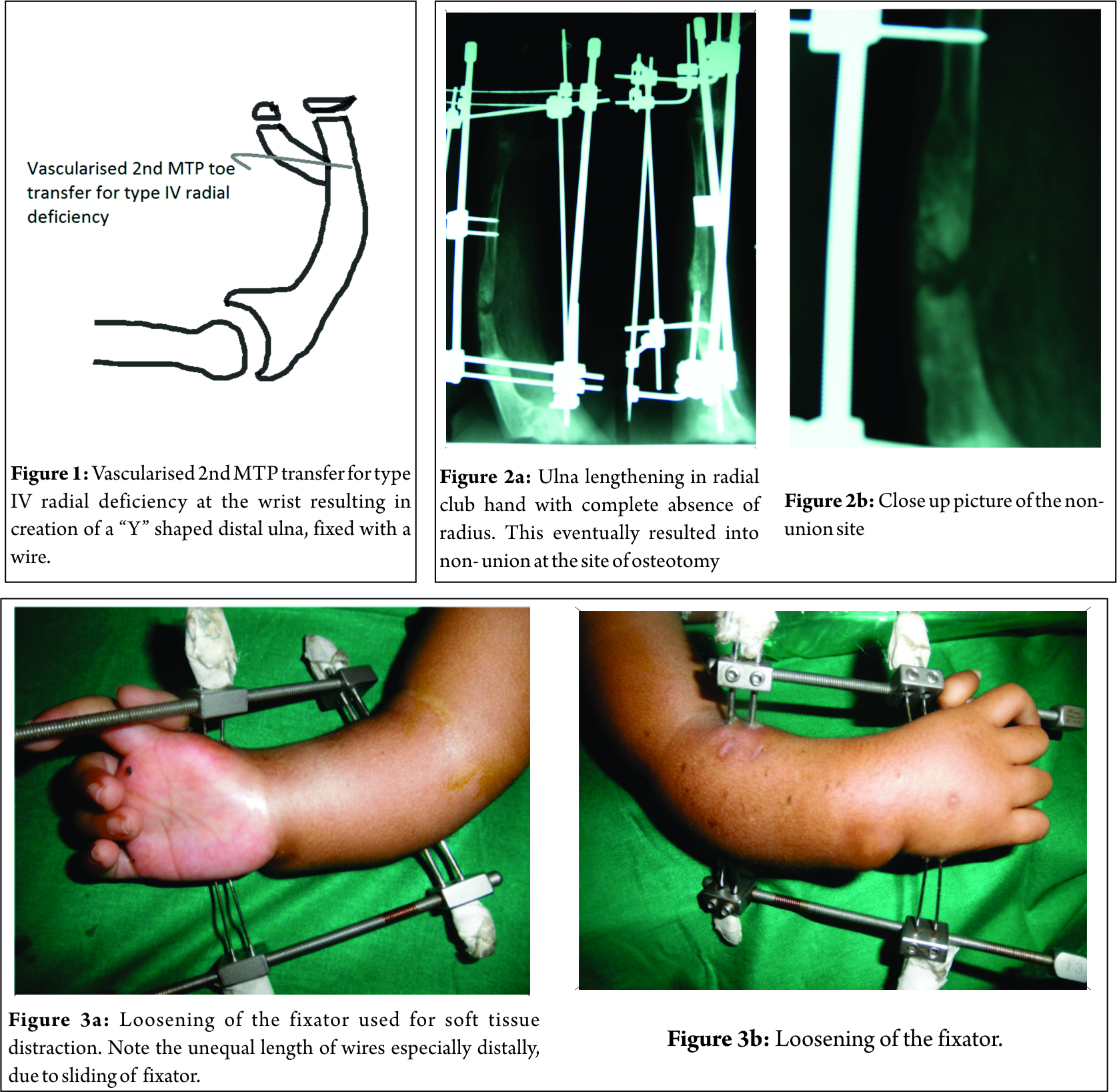
Vilkki [20] used a novel technique for treatment of Bayne type III and IV radial deficiency using the 2nd MTP joint as a vascularized graft to create a radial column within the wrist (see Fig. 1). The metatarsal and proximal phalanx of the 2nd toe are transferred to the forearm to create a Y shaped distal ulna with potential for growth at both limbs of “Y”. He used a monolateral external fixator in conjunction with this. With regard to the design of the external fixator, the author commented, ‘‘the lengthening device can still be improved and it should have the potential to correct angular deformities.’’ The author also acknowledged unpredictable growth of the transferred bone, cosmetic concerns of the transferred skin pedicle, and technical difficulties with microvascular transfer. Residual radial deviation of the wrist averaging 200 was noted at follow-up. One patient developed a traumatic fracture of the transplanted joint. Consequently the treatment protocol was adjusted to using the distraction device for at least nine weeks following MTP transfer.
Vilkki [13] reported the long term results of vascularized second metatarsophalangeal joint on 24 limbs with an average follow-up of 11 years. The average radial deviation at final follow- up was 280, the average active wrist total arc of motion was 830, and the average length of the ulna was 67% of the contralateral side. Complications were present in more than 50% of patients, including 5 cases of failure of the transfer, 2 of which were vascular in origin and 3 of which had necrosis or fracture leading to necrosis of the metatarsal head. Subluxation of the joint was present in 6 cases and several patients underwent subsequent osteotomies or joint transfer procedures. Distractor device complications was present in 2 patients, fracture of the MTP joint in 2 patients, delayed bony union of the metatarsal ulna interface in 2 patients and pseudoarthrosis at the MTP joint in 2 patients. Three children required late joint transport to lengthen MTP constructs that failed to grow adequately. Donor site morbidity was noted in only 4 patients with hallux valgus noted in one patient, prominent scarring in 2 and occasional pain noted in one other.
These findings of ulna length compares favorably with previous reports of Sestero et al. [7] who found that untreated limbs of patients with radial club hand grew to 64% of normal ulnar length, while surgically centralized limbs within their study grew to only 48-58% of normal ulnar length.
The evidence regarding treatment of radial deficiency of the forearm is limited to retrospective case series. The wide variation in types of operative treatment reflects the lack of a clearly superior procedure. All options have high rates of recurrence with the potential for multiple procedures, all of which have considerable complication rates.
Conclusion
Strategies suggested by the authors for preventing complications are as follows:
1. Good volar and radial skin release
2. Accurate reduction of carpus on ulna
3. Good soft tissue repair
4. Tendon balancing
5. Tightening of structures on ulnar side
6. Temporary stabilization of carpus on ulna
7. Distraction of carpus on ulna (when required with a careful watch to prevent physeal distraction)
8. Limited lengthening of ulna restricted to at the most 5 centimeters in one stage. Elbow stability is an important pre-operative consideration, given that sometimes there may be a co-existing shallow olecranon fossa.
References
1. Flatt AE. The Care of Congenital Hand Anomalies, 2d ed. St Louis: Quality Medical Publishing, 1994:366–410.
2. Urban MA, Osterman LA. Management of radial dysplasia. Hand Clin. 1990;6:589–605.
3. Buck-Gramcko D. Radialization as a new treatment for radial club hand. J Hand Surg [Am]. 1985;10:964–968.
4. Lamb DW. Radial club hand. J Bone Joint Surg [Am]. 1977;59:1–13.
5. Watson HK, Beebe RD, Cruz NI. A centralization procedure for radial clubhand. J Hand Surg [Am]. 1984;9: 541–547.
6. Bayne LG, Klug MS. Long-term review of the surgical treatment of radial deficiencies. J Hand Surg [Am]. 1987;12: 169–179
7. Sestero AM, Van Heest A, Agel J. Ulnar growth patterns in radial longitudinal deficiency. J Hand Surg Am. 2006;31(6):960–967. [PubMed]
8. Shariatzadeh H, Jafari D, Taheri H, Mazhar FN. Recurrence rate after radial club hand surgery in long term follow up. J Res Med Sci. 2009;14(3):179–186
9. Lamb DW, Scott H, Lam WL, Gillespie WJ, Hooper G. Operativecorrection of radial club hand: a long-term followupof centralization of the hand on the ulna. J Hand Surg Br.1997;22(4):533-6.
10. Damore E, Kozin SH, Thoder JJ, Porter S. The recurrence of deformity after surgical centralization for radial clubhand. J Hand Surg Am. 2000;25(4):745e751
11. Heikel HV. Aplasia and hypoplasa of the radius: studies on 64 cases and on epiphyseal transplantation in rabbits with the imitated defect. ActaOrthopScand Suppl. 1959;39:1- 155.
12. Goldfarb CA, Klepps SJ, Dailey LA, Manske PR. Functional outcome after centralization for radius dysplasia. J Hand Surg Am. 2002;27(1):118–124.
13. Vilkki SK. Vascularised metatarsophalangeal joint transfer for radial hypoplasia. Semin Plastic Surgery.2008; 22(3): 195- 212
14. C. Romanaa, G. Ciaisa, F. Fitoussi. Treatment of severe radial club hand by distraction using an articulated mini-rail fixator and transfixing pins. Orthopaedics& Traumatology: Surgery & Research Volume 101, Issue 4, June 2015, Pages 495–500
15. Pike JM, Manske PR, Steffen JA, Goldfarb CA. Ulnocarpal epiphyseal arthrodesis for recurrent deformity after centralization for radial longitudinal deficiency. J Hand Surg Am. 2010;35(11): 1755- 1761.
16. Farr S, Petje G, Sadoghi P, Ganger R, Grill F, Girsch W. Radiographic early to midterm results of distraction osteogenesis in radial longitudinal deficiency. J Hand Surg Am. 2012;37(11): 2313-2319.
17. Peterson BM, McCarroll HR Jr, James MA. Distraction lengthening of the ulna in children with radial longitudinal deficiency. J Hand Surg Am. 2007;32 (9):1402-1407.
18. Yoshida K, Kawabata H, Wada M. Growth of the ulna after repeated bone lengthening in radial longitudinal deficiency. J PediatrOrthop. 2011;31(6):674e678.
19. Matsuno T, Ishida O, Sunagawa T, Suzuki O, Ikuta Y, Ochi M. Radius lengthening for the treatment of Bayne and Klug type II and III radial longitudinal deficiency. J Hand Surg Am 2006;31 (5): 822- 829
20. Vilkki SK. Distraction and microvascular epiphysis transfer for radial club hand. J Hand Surg [Br]. 1998;23: 445–452.
| How to Cite this Article: Maheshwari R, Mehta R, Johari AN. Complications of Surgical Management of Radial Club Hand. International Journal of Paediatric Orthopaedics Sep-Dec 2016;2(3):24-27. |