The Effect of Guided Growth on Rotational Deformities of the Long Bones: A Biomechanical Study on Sawbone
Vol 1 | Issue 1 | July-Sep 2015 | page:44-47 | Emre Cullu, Mutlu Cobanoglu, Mustafa Kemal Peker.
Authors : Emre Cullu[1], Mutlu Cobanoglu[2*], Mustafa Kemal Peker[3].
[1] Adnan Menderes University Medical School, Deparment of Orthopaedics and Traumatology,
Turkey.
Address of Correspondence
Dr. Mutlu Cobanoglu
Adnan Menderes University Medical School, Department of Orthopaedics and Traumatology, KepezMevkii 09100 Aydın / Turkey
E-mail: drmutlu79@hotmail.com
Abstract
Background: Although temporary hemi-epiphysiodesis is an effective method for correction of frontal and sagittal plane limb deformity in growing children, osteotomy is commonly performed to correct rotational deformities of the long bones. The aim of this report is to improve rotational guided growth with a formula created to calculate the amount of correction.
Methods: A femur sawbone was cut above the trochlear sulcus. Two 8-plates were placed opposite to each other on medial and lateral sides of the cutting line. Three pairs of holes were drilled in three different angles on medial side and lateral side to place two plates on sawbone. The bone was distracted by an intramedullary device. The anteversion angles were measured by computerized tomography. The angles between the femoral axis and the plates were measured on X-ray. A formula was used to calculate the amount of correction.
Results: As the bone was distracted, rotation of the distal part of the cutting line was observed. When the angles between the plates and the long axis of the bone (α) were 50°, 36°, and 26°, the axial rotations were -11.25°, 2.43°, and 7.06° respectively on CT. When the formula was applied, the amounts of corrections were 25.7°, 18.5°, and 13.4° respectively.
Conclusions: This study supports that this technique can be used for correction of rotational deformities of the long bones. It’s said that the wider angle between the plates and the long axis of the bone, the greater rotation. But further experimental studies are required to improve this technique.
Keywords: Rotational guided growth, rotational deformity, temporary epiphysiodesis.
Introduction
There are many options for the correction of angular bone deformities but the standard treatment has been osteotomy. Currently, hemi-epiphysiodesis is considered an effective treatment to correct an axial limb deformity in children [1,2] and Stevens presented a technique using an 8-plate [3]. Although this technique is an effective treatment method for correction of frontal and sagittal plane limb deformities in growing children, osteotomy is still a commonly used surgical technique for rotational deformities of the long bones. In the recent years, it has been thought that a rotational deformity in the horizontal plane of the long bones could be corrected by guided growth and two animal studies, which evaluated guiding rotational growth, were published [4,5]. In this biomechanical study the aim was to improve rotational guided growth with a formula created to calculate the amount of correction. Because of that a sawbone model was designed.
Materials and Methods
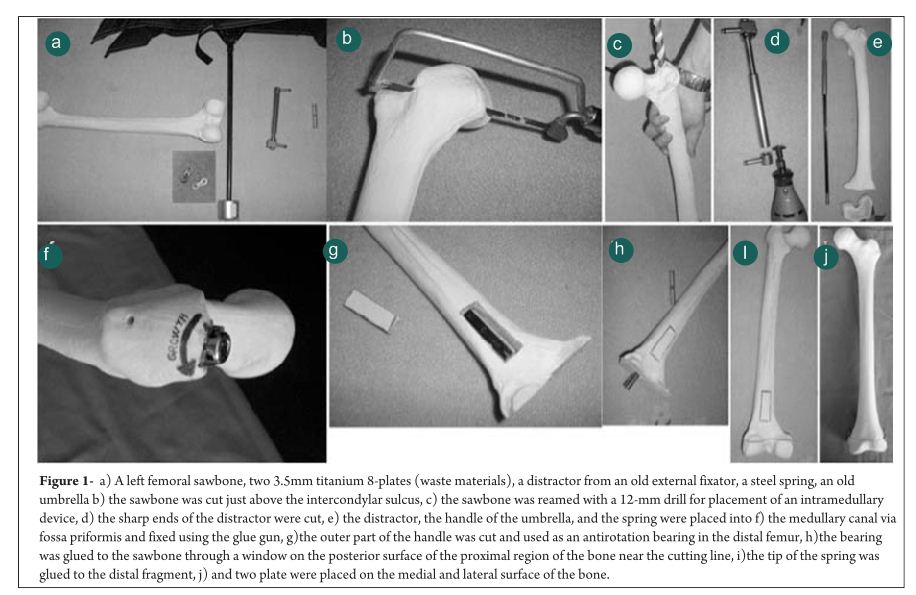
One femur foam cortical shell sawbone with a 15 mm diameter canal and 42 cm overall length was used for the model. A left femoral sawbone, two titanium growth 8-plates (Biomet/USA and TST/Turkey), a distractor of an external fixator, a steel spring, a handle of an umbrella were used to construct this model. The sawbone was cut just above the intercondylar sulcus. This cutting line acted as a physeal line. The sawbone was reamed from the fossa priformis with a 12-mm drill for the placement of an intramedullary device to distract the fragments. The sharp ends of the distractor were cut. The distractor, the handle of the umbrella, and the spring were placed into the medullary canal via fossa priformis and fixed with glue gun. The outer part of the handle was cut and used as an antirotation block in the canal. The block was glued to the sawbone through a window opened from posterior surface of the proximal side of the cutting line. This block prevented the rotation of the distractor in the canal. The tip of the spring was fixed with glu to the distal fragment. This spring was placed between proximal and distal fragments. When the device was distracted, the device pushed the spring toward the distal fragment. By this way the lengthening was obtained. Because of the spring, distractor did not create an external rotation force on the distal fragment by itself directly (Figure 1).
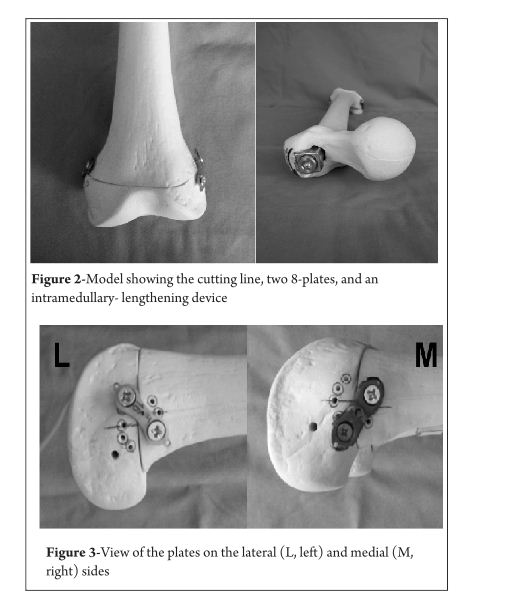
Three pairs of holes were drilled in three different angles to place plates on the sawbone, Two 8-plates, whose brands were different, with four screws were used to fix the cutting line and were placed on medial and lateral side of the bone (Fig 2). The different plates of different brands were helpful to differentiate one plate from the other on lateral X-ray. To create external rotation the medial plate was placed obliquely from the proximal anterior region to the distal posterior region, and the lateral plate was placed obliquely from the proximal posterior region to the distal anterior region (Figure 3).
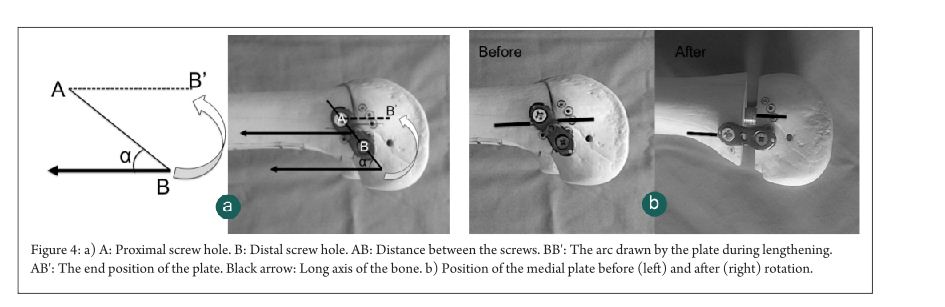
Fixation of the plates was performed in three different angles. The screws were not tightened completely. An allen wrench was used to distract the intramedullary device on its proximal end. The distances between proximal and distal holes were measured in each plate manually. The angles between the femoral axis and the plates were measured on lateral X-ray. Femoral length (FL) (from the tip of trochanter major to top of intercondylar notch), mechanical lateral distal femoral angle (mLDFA), anatomic posterior distal femoral angle (aPFDA) were evaluated on computerized tomography (CT) scanogram. The femoral anteversion of the sawbone was measured on CT. A flat surface was used to immobilize the sawbone and to standardize the evaluation of the rotation. Retroversion was defined as negative value, anteversion was defined as positive value. All parameters were evaluated on PACS (Picture Archiving and Communication System) radiologic system. A formula was created to calculate that how many degrees the plates should be placed to obtain desired amount of rotation. Depending on the length and angle of the plates, the arc length scanned by the plate was equal to the arc length scanned by the distal fragment until the plate became horizontally. Additionally, the arc length scanned by the distal fragment depended on its radius. The length of the arc (the distance between the first position (B) and the last position (B’) of the distal screw of the medial plate) swept by the plate is equal to the path drawn by the rotation around its axis of the distal region (Figure 4).
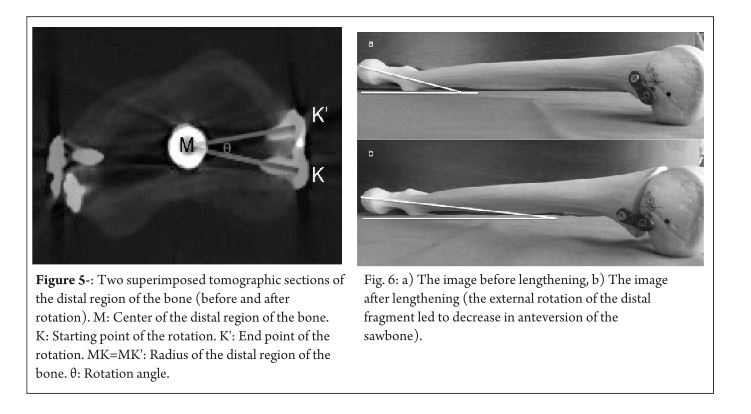
The virtually spiral movement of this region along the axis is shown as the progress of the arc on the surface of the cylinder (Figure 5). A full rotation of the arc of the helix is equal to the diagonal line of the open shape of the cylinder.
The formula which was created to calculate the amount of correction (θ) is demontrated as follows:
BB’ 2Π·ΑΒ·α/360
KK’ 2Π· MK·θ/360
BB’KK’
2Π·ΑΒ·α/360 2Π·MK·θ/360
θ ΑΒ·α /MK
(A: Position of the proximal screw of the medial plate, B: The first position of the distal screw of the medial plate, B’: The last position of the distal screw of the medial plate, α: The angle between long axis of the sawbone and medial plate, M: Center of the distal region of the bone. K: Starting point of the rotation. K’: End point of the rotation. MK=MK’: Radius of the distal region of the bone. θ: Rotation angle)
Results
The FL was 421.79 mm and the anteversion of the sawbone was 8.26° before distraction. When the sawbone was distracted, rotation of the distal fragment was observed without translation (Figure 6). When the angles between the plates and the long axis of the bone (α) were 50°, 36°, and 26°, the axial rotations were -11.25°, 2.43°, and 7.06° respectively on CT and the FLs were 433.38mm, 430.02mm, 429.74mm respectively after full distraction. Thus, the amount of correction (θ) were 19.25°, 5.83°, and 1.20°, respectively. The wider the angle between the plates and the long axis of the bone, the more rotation and lengthening occurred. As the screws were not tightened completely, rotation of the plates, which led to more rotation of the distal fragment and lengthening of the bone, occurred more easily.
In the coronal plane, mLDFA was 87° before lengthening. After lengthening mLDFAs were constant when the α angle were 50° and 36°. But mLDFA was 83° when the α was 26°.
In the sagittal plane, aPDFA was 89° before lengthening. After lengthening aPDFAs were 90° when the α angles were 50° and 36° and aPDFA was 91° when the α angle was 26°.
The distance between the screw holes (AB) was 18 mm, and the radius of the distal fragment of the femur (MK) was 35 mm. When the formula was used, the amounts of correction (θ) were 25.7°, 18.5°, and 13.4°, respectively. None of the calculated degrees of correction were comparable to the CT measurements.
Discussion
Angular deformities around the knee can be corrected with hemiepiphysiodeses in skeletally immature patients [2,6,7]. The epiphysis grows symmetrically under normal conditions. If the physeal plate is compressed from one side, an angular deformity can occur. Mechanical modulation of longitudinal growth by compressive forces is a widely accepted notion, also known as the Volkmann’s law [8]. However, osteotomy is the most commonly used surgical technique for the correction of rotational deformities of the long bones. Furthermore, rotational guided growth are not currently used to correct rotational deformities of the long bones in clinical practise. There are two reported animal studies [4,5]. Arami et al used rabbit femur in their study and to induce external rotation the distal part of the medial plate was positioned posteriorly and to induce internal rotation the distal part of the medial plate was positioned anteriorly. They said that because of the shape of the medial femoral condyle, some technical difficulties occurred and medial plate was placed in desired position in the group of external rotation [4]. The physeal line of the distal femur of rabbit is wavy and not straight. For this reason to place both plates obliquely in different directions on wavy line is not seen feasible. Firstly more straight physeal line is needed. Cobanoglu et al studied on the proximal tibial epiphysis of rabbit to induce external rotation. The reason why they preferred proximal tibia to distal femur could be that the proximal tibia had straighter physeal line than distal femur. They only studied on external rotation group and did not create a formula about prediction amount of rotation [5]. This study is a biomechanical study. And the aim of this study is to create a formula based on the angle between the long axis of the bone and the plates. A distal femoral physeal plate was created by cutting the sawbone just above the trochlear sulcus and two 8-plates were placed on either side of the cutting line. It was thought that if two plates were placed at reverse angles to each other on either side of the bone, the distal fragment would be rotated. According to this theory, the screws in the holes should not be tightened completely to create rotation points or free zones between the plates and screws. These rotation points would cause the plates to spin around the screws like a hinge. The screws were placed as closely as possible to the cutting line, and thus the plate placement angle was increased. We used an intramedullary device to distract the bone. While the sawbone was being distracted, rotation of the distal fragment was obtained and this led to a reduction in the anteversion of the femur due to the placement of the plates. The upper limit of rotation which can be corrected, is due to orientation of the plates and the distance between the proximal and the distal screws. Therefore, insertion of these plates with the greatest angle to the long axis as possible and the greatest distance between the screws as possible will lead greater rotation. These are two important variables in the formula. These variables are related to anatomical properties of the bone such as width and points for plate fixation. The angle between the positions of the plate and the bone axis needs monitoring. For this reason, the position of the plates at the end of the rotational correction is crucial to prevent angular deformities. The important points of this technique are the distance between the proximal and distal screws and the tightness of the screws. The use of long plates results in greater lengthening and rotation, depending on the distance between the holes. When the distance between the proximal and distal screws is as great as possible, increased gap between the fragments and more rotation of the distal fragment are observed. And to be able to obtain rotation of the plate more easily, the screws must not be tightened completely. Another important point is that placement of the plates at the same angle onto the bone. For this reason, the amount of rotation will reveal according to the plate having less angle with bone axis. When the axis of this plate is parallel to the bone axis, the plate will not rotate and causes a deformity. So the deformities of the condyles can affect the rotational measure. Arami et al used inter-plate angle in their study and declared that every 1° of change in this angle corresponded 0.378° of rotational profile difference [4]. In our opinion because of the reasons mentioned above, the rotational profile is dependent on the angle between the plate and bone axis, not inter-plate angle. The CT measurements and calculations using the formula differed from each other. There are three possible reasons for this disparity: First, there was laxity between the screws and the plates, leading to instability between the proximal and distal regions of the sawbone. Second, the sawbone had a circular structure whereas the plates were straight. These incompatible shapes might prevent rotation. Third, the distal region of the bone does not form a precise circle. This technique has not been performed to humans yet. This biomechanical study supports that this technique can be used for the correction of rotational deformities of the long bones. It’s said that the wider angle between the plates and the long axis of the bone, the greater rotation. But further animal studies are required to demonstrate efficacy of this hypothesis.
References
1. Houshian S, Mehdi B, Larsen MS. The epidemiology of elbow fracture in children: analysis of 355 fractures, with special reference to supracondylar humerus fractures. J Orthop Sci 2001;6(4):312-5
2. Barr LV. Pediatric supracondylar humeral fractures: epidemiology, mechanisms and incidence during school holidays. J Child Orthop. 2014; 8:167–170
3. Cheng, Jack CY, Ng, BKW, Ying, S. Y, Phil P. A 10-Year Study of the Changes in the Pattern and Treatment of 6,493 Fractures. 19(3), May/June 1999, pp 344-350
4. Kemp AM, Dunstan F, Harrison S, Morris S, Mann M, Rolfe K, Datta S, Thomas DP, Sibert JR, Maguire S. Patterns of skeletal fractures in child abuse: systematic review. BMJ 2008; 337:a1518
5. Strait RT, Siegel RM, Shapiro RA. Humeral fractures without obvious etiologies in children less than 3 years of age: when is it abuse? Pediatrics. 1995 Oct;96(4 Pt 1):667-71
6. Cheng JC, Lam TP, Maffulli N. Epidemiological features of supracondylar fractures of the humerus in Chinese children. J Pediatr Orthop B 2001;10(1):63-67
7. Mahan SD, May CD, Kocher MS. Operative Management of Displaced Flexion Supracondylar Humerus Fractures in Children. J Pediatr Orthop 2007;27:551-556
8. Leitch KK, Kay RM, Femino JD, Tolo VT, Storer SK, Skaggs DL. Treatment of multidirectionally unstable supracondylar humeral fractures in children. A modified Gartland type-IV fracture. J Bone Joint Surg Am. 2006 May;88(5):980-5.
9. Skaggs DL, Flynn JM. (2010) In Rockwood and Wilkins’ Fractures in Children. Philadelphia. Lippincott Williams and Wilkins. 514-515
10. Bahk MS, Srikumaran U, Ain MC, Erkula G, Leet AI, Sargent MC, Sponseller PD. Patterns of Pediatric Supracondylar Humerus Fractures. J Pediatr Orthop 2008;28:493-499.
11. Sen RK, Tripathy SK, Kumar A, Agarwal A, Aggarwal S, Dhatt S. Metaphyseo-diaphyseal junction fracture of distal humerus in children.
J Pediatr Orthop B 2012, 21:109–114
12. Blount WP. Fractures in Children. Baltimore: Williams and Wilkins, 1955
13. France J, Strong M. Deformity and function in supracondylar fractures of the humerus in children variously treated by closed reduction and splinting, traction and percutaneous pinning. J Pediatr Orthop. 1992:12(4): 494-498
14. Khoshbin A, Leroux T, Wasserstein D, Wolfstadt J, Law PW, Mahomed N, Wright JG. The epidemiology of paediatric supracondylar fracture fixation: A population-based study. Injury. 2014; 45: 701–708Khoshbin A, Leroux T, Wasserstein D, Wolfstadt J, Law PW, Mahomed N, Wright JG. The epidemiology of paediatric supracondylar fracture fixation: A population-based study. Injury. 2014; 45: 701–708
15. Kasser JR. Location of treatment of supracondylar fractures of the humerus in children. Clin Orthop Relat Res. 2005 May;(434):110-3
16. Slobogean BL, Jackman H, Tennant S, Slobogean GP, Mulpuri K. Iatrogenic ulnar nerve injury after the surgical treatment of displaced supracondylar fractures of the humerus: number needed to harm, a systematic review. J Pediatr Orthop 2010;30(5):430-6
17. Lyons, James P. M.D.; Ashley, Edwin M.D.; Hoffer, M. Mark M.D. Ulnar Nerve Palsies After Percutaneous Cross-Pinning of Supracondylar Fractures in Children’s Elbows. J Pediatr Orthop. 1998:18, 43-45
18. Lee YH, Lee SK, Kim BS, Chung MS, Baek GH, Gong HS, Lee JK. Three Lateral Divergent or Parallel Pin Fixations for the Treatment of Displaced Supracondylar Humerus Fractures in Children. J Pediatr Orthop 2008;28:417-422
19. Kocher MS1, Kasser JR, Waters PM, Bae D, Snyder BD, Hresko MT, Hedequist D, Karlin L, Kim YJ, Murray MM, Millis MB, Emans JB, Dichtel L, Matheney T, Lee BM. Lateral entry compared with medial and lateral entry pin fixation for completely displaced supracondylar humeral fractures in children. A randomized clinical trial. J Bone Joint Surg 2007;89(4):706-12
20. Mahan ST, Osborn E, Bae DS, Waters PM, Kasser JR, Kocher MS, Snyder BD, Hresko MT. Changing Practice Patterns: The Impact of a Randomized Clinical Trial on Surgeons Preference for Treatment
of Type 3 Supracondylar Humerus Fractures. J Pediatr Orthop 2012;32:340–345
21. Battaglia TC, Armstrong DG, Schwend RM. Factors affecting forearm compartment pressures in children with supracondylar fracture of the humerus. J Pediatr Orthop. 2002; 22(4): 431-439
22. Blackmore LC, Cooperman DR, Thompson GH. Compartment syndrome in ipsilateral humerus and forearm fractures in children. Clin Orthop and Relat Res. 2000; 376: 32-38
23. Campbell CC, Waters PM, Emams JB, Kasser JR, Millis MB. Neurovascular injury and displacement in type 3 supracondylar humerus fractures. J Pediatr Orthop. 1995;15(1):47-52
24. Choi PD, Melikian R. Skaggs DL. Risk Factors for vascular repair and compartment syndrome in the pulseless supracondylar humerus fracture in children. J Pediatr Orthop 2010;30:50-56
.
| How to Cite this Article: Cullu E, Cobanoglu M, Peker MK. The Effect of Guided Growth on Rotational Deformities of the Long Bones: A Biomechanical Study on Sawbone. International Journal of Paediatric Orthopaedics July-Sep 2015;1(1):44-47. |