
Pollicisation: Embryology, History, Technique and Results
Volume 2 | Issue 2 | May-Aug 2016 | Page 29-33|Amita S. Hiremath, Binita N. Raut, Amit A. Yadav, Mukund R. Thatte
Authors :Amita S. Hiremath [2], Binita N. Raut [1], Amit A. Yadav [2], Mukund R. Thatte [3]
[1] KLE University’s J.N.Medical College,Belgavi,
[2] Bombay Hospital and Institute of Medical Sciences Mumbai.
[3] Bombay Hospital and Institute of Medical Sciences Bai Jerbai Wadia Hospital for Children, Shushrusha Citizens’ Co‑op. Hospital,Maharashtra, India
Address of Correspondence
Dr Mukund R. Thatte, Room 6, 2nd Floor, New Wing, Bombay Hospital, New Marine Lines, Mumbai ‑.400 020, Maharashtra, India.
E‑mail: mthatte@gmail.com
Abstract
Thumb hypoplasia/aplasia is one of the components of radial longitudinal deficiency. It can occur either alone or it may be associated with other components of radial longitudinal deficiency. Aim of thumb reconstruction is to provide a functional and stable thumb which will improve the grip and aesthetic appearance of hand. Pollicisation is the treatment for Type IIIB,IIIC, IV and V types of thumb hypoplasia as per Blauth’s Classification as Modified by Manske and Buck-Gramcko. In the opinion of the authors, pollicisation is one of the finest and most difficult operations in reconstructive hand surgery.
Keywords: Pollicisation: History, Principles and Surgical technique.
Introduction
Napier has said “The hand without a thumb is at worst, nothing but an animated fish-slice, and at best a pair of forceps whose points don’t meet properly”. [1]
Thumb hypoplasia is a congenital condition, which can range from slightly small digit to deficiency of some musculotendinous units or osseous components to complete absence of thumb.40% of the hand function relies on a strong thumb. [2]For proper functioning of the hand, thumb size, its position,mobility and the relation with other fingers is critical. Children with thumb hypoplasia can manipulate small objects using side to side pinch, between adjacent digits, ‘Chopstick’ action; but it is difficult to grasp large objects. [3]
Thumb hypoplasia/aplasia is one of the components of radial longitudinal deficiency. It can occur either alone or it may be associated with other components of radial longitudinal deficiency. A wide range of manifestations on the preaxial side of the upper limb is seen in radial longitudinal deficiency. Hence, in any case of thumb hypoplasia, one should examine proximal forearm and contralateral thumb.
Incidence
Thumb hypoplasia is a component of various congenital malformations like thumb duplication, transverse deficiencies, brachydactyly, symbrachydactyly, cleft hand complex, constriction ring syndrome etc., and hence it is very difficult to find out the true incidence of thumb hypoplasia alone. Tay SC et al in 2006, reported upto 16% incidence of thumb hypoplasia amongst congenital hand deformities. [4] There is equal distribution of cases between male and female. About 60% cases have bilateral involvement with often asymmetrical involvement. [5] In unilateral cases, right hand is more commonly affected. [6]
In a study by Abdel-Ghani and Amro, [7] 86% cases of thumb hypoplasia were associated with various conditions involving cardiovascular, gastrointestinal and genitourinary system. Various conditions commonly seen in association with thumb hypoplasia are Holt-Oram syndrome, VACTERL association, Fanconi’s anaemia, Thrombocytopenia absent radius(TAR) syndrome. [6] The severity of radial longitudinal deficiency is directly proportional to the degree of thumb hypoplasia according to James et al. [8]
Genetics
The upper limb bud appears at 4th week of embryonic development opposite the caudal cervical somites. Various signalling centres have been identified that are responsible for upper limb development. [4,8]
1. Apical Epidermal Ridge(AER) – responsible for proximal to distal development (shoulder to hand) and is mediated by number of fibroblast growth factors.
2. Zone of Polarizing Activity (ZPA) – responsible for anterior-posterior pattern formation(also called Pre and Post Axial) and is mediated by sonic hedgehog (Shh) and homeobox (HOX) gene products.
3. WNT7a signalling centre – responsible for dorsal ventral development.
The exact mechanism of embryologic insult that leads to thumb hypoplasia is unclear. Abnormalities in AER or ZPA can lead to thumb hypoplasia. Studies have proved that administration of teratogenic agents or inactivating fibroblastic growth factors in rats and mice can lead to radial longitudinal hypoplasia with thumb hypoplasia. [10]
The deletion of chromosome 22q11 can lead to thumb hypoplasia in radial longitudinal deficiency [5]. However, it is difficult to point out single gene or enzymatic defect as the cause for thumb hypoplasia [8].
Classification
Thumb hypoplasia can present with wide range of functional and aesthetic differences. Hence careful inspection and examination is required. One should carefully examine the size, position, skeletal components, intrinsic and extrinsic muscles, joint stability, and first web space and associated conditions. One should correlate soft tissue and skeletal deficiencies while taking decision about the treatment.
Classification helps in taking decision about the treatment. In 1937, Muller first classified thumb hypoplasia. It is currently the Blauth’s classification which is widely accepted in classifying and as a guide for surgical planning. Manske further classified type 3 hypoplasia in A and B depending on stability of CMC joint. [4, 11]
Blauth’s Classification as Modified by Manske and Buck-Gramcko:
Type I: Mild hypoplasia
Slight decrease in thumb size
Slender phalanges and metacarpals
Normal intrinsic muscles
Normal trapezium, scaphoid, distal radius and styloid process
Type II: Moderate hypoplasia
Underdeveloped or absent thenar muscles
Adducted posture- first web space narrowing
Ulnar Collateral ligament (UCL) insufficiency at MP joint
CMC stable
Type III: Severe hypoplasia
All the features of type II plus
Radial carpal aplasia
Extrinsic muscle and tendon abnormalities
Type III A: Stable CMC joint
Type III B: Unstable CMC joint
Type IIIC: Buck Gramcko has added this variation in which thumb has only metacarpal with no musculotendinous unit and a wider skin bridge
Type IV: Pouce floutant (French Floating thumb)
Thumb is small and has rudimentary skeletal elements. It is an unstable digit, connected to the hand by only a skin bridge containing the neurovascular bundle.
Type V: Aplasia i.e.Absence of all thumb structures and radial carpal bones
 Figure 1: Preoperative picture of Type IV thumb hypoplasia (volar view) |
") Figure 2: Preoperative picture of Type IV thumb hypoplasia (dorsal view) |

Figure 3: Preoperative xray showing rudimentary skeletal elements
Evaluation
Thumb hypoplasia can be the only presentation of radial longitudinal deficiency or it may be associated with other anomalies. Plain bilateral radiographs will help to assess thumb phalanges, metacarpal and carpometacarpal joint. One should assess wrist and forearm to rule out radial longitudinal deficiency.
As thumb hypoplasia can be associated with other syndromes, thorough cardiac, renal, haematological and musculoskeletal evaluation is essential. Common investigations include a complete blood count, 2D Echo Cardiogram and sonography abdomen for solid organs. This is important as the treatment of these conditions may take priority over thumb hypoplasia management. [12]Any positive findings may also impact anaesthesia for surgery.
 Figure 4: Buck Gramcko type markings for dorsal side |
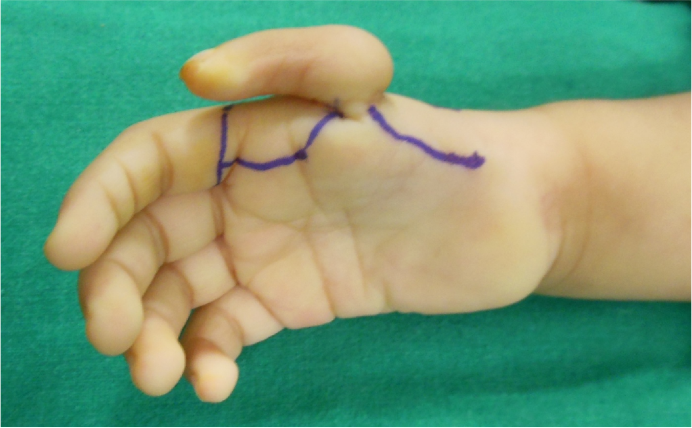 Figure 5: Buck Gramcko type markings for palmar side |
 Figure 6: Dorsal flaps raised preserving dorsal venous network |
Treatment
Aim of thumb reconstruction is to provide a functional and stable thumb which will improve the grip and aesthetic appearance of hand.
Typically Type I is more or less a functional thumb,hence no treatment is required.
Type II: depending on findings; first web space release, opponensplasty using Abductor Digiti Minimi (ADM) or other suitable donors and/or UCL reconstruction
Type III A: same procedures like type II and in addition may require further additional extrinsic tendon transfers to improve the function, which transfers and how needs to be decided on a case by case basis, depending on need.
Type IIIB,IIIC, IV and V: Pollicisation
Timing of surgery:
Surgery at an early age is recommended for better functional results as it will allow cognitive development and physiological adaptation of the reconstructed thumb before corticalisation which happens around 18 months of age. [13]
We are basically going to discuss about pollicisation in advanced hypoplasia IIIB onwards or Aplasia in this paper.
Pollicisation is a Latin word; Pollex means thumb and Pollicisation is defined as reconstruction of thumb using the adjacent radial finger.
History of pollicisation
In 1885,Guermonprez seems to be the first person to report a case of pollicisation. Before the second world war, many surgeons Dunlop (1923), Bunnell (1931) have reported doing pollicisation. However, follow up study of these cases had unsatisfactory results.
The major modification in the procedure was seen after the Second World War. Gosset (1949) [14] described index finger and ring finger pollicisation on neurovascular pedicle without skin attachments. Middle finger pollicisation was described by Hilgenfeldt (1950) [15]. Further contributions were by Bunnell (1952), Littler (1953). [16.17]
In 1971, Buck Gramcko published an article about pollicisation [18] which is the landmark article in establishing the technique of pollicisation in our opinion. Buck Gramcko’s major work on pollicisation evolved after the thalidomide tragedy in Europe which had led to many congenital hand and upper limb anomalies. Manske, Foucher et all have modified the technique but Buck Gramcko’s technique is the gold standard method still commonly used. The authors use the Buck Gramcko technique.
Principles of Pollicisation:
In 1990 Littler had said:
“It is not the full length of the thumb, nor its great strength and movement, but rather its strategic position relative to the fingers and the integrity of the specialized terminal pulp tissue which determines the prehensile status.”
Littler has classified requirements of the procedure as follows [19]
Mechanical
1. Correct length
2. Strategic position
3. Stability
Physiological
1. Movement
2. Sensibility
3. Absence of pain
4. Integration
Satisfactory appearance
In the opinion of the authors, pollicisation is one of the finest and most difficult operations in reconstructive hand surgery. Patient’s parents have a tough time deciding about amputing the useless thumb and using index finger for thumb reconstruction. Authors feel it is simultaneously rewarding to and taxing on the surgeon performing it. [20]
TECHNIQUE Figs. 1- 17
Fig. 1,2 and 3 represent pre operative photos and X-Ray.
Markings as per Buck-Gramcko (Fig. 4,5) Senior author (MRT) starts the surgery by raising the dorsal flaps taking care to preserve dorsal venous network. (Fig. 6)
Once the dorsal flaps are raised preserving dorsal venous network, palmar incisions are made and pedicles are dissected on the palmar side. Sometimes it may be required to open the neural ring on the ulnar side pedicle,if it is present.(Fig.7)

Figure 7: Dissection of vascular pedicles of Index finger
After dissecting and safeguarding the pedicle, first dorsal interosseous and first palmar interosseous with lateral band extension is identified and cut. To identify the distal lateral band at the time of final suturing, a 6-0 nylon suture is used for tagging the remaining lateral band (Fig. 8,9,10)
 Figure 8: First dorsal interroseous raised with tendon |
 Figure 9: Lateral band on finger tagged with 6/0 nylon loose stitch for later identification |
 Figure 10: First palmar interroseous raised with tendon |
Next step is to identify the two extensors – extensor indicis proprius and extensor digitorum communis of index finger and cut them. In more severe variants of Radial dysplasia only one tendon is present.(Fig. 11)

Figure 11: Extensor digitorum communis and Extensor Indicis proprious seen
 cut and raised off MP joint so as to act on distal interphalangeal as future extensor pollicis longus")
Figure 12: Extensor Indicis proprious (EIP) cut and raised off MP joint so as to act on distal interphalangeal as future extensor pollicis longus
For setting the index completely free, the deep transverse metacarpal ligament between index and middle finger has to be divided. (Fig. 13)

Figure 13: Dividing deep transverse metacarpal ligament between index and middle finger
The line of division of metacarpal is through the epiphysis at the level of the head. The shaft is disarticulated at the CMC joint and is excised extra-periosteally.(Fig. 14,15)
 Figure 14: Division of index finger metacarpal at the level of head of metacarpal |
 Figure 15: Metacarpal shaft disarticulated at carpometacarpal joint |
At every step, one has to be careful about the neurovascular pedicle of the index finger.
The metacarpal head has to be rotated by 900 in extension and fixed with 4-0 nylon to prevent hyperextension of the new CMC joint.(Fig 16)

Figure 16: Rotating metacarpal head dorsally by 900
Index finger is now rotated 150 degrees, abducted 40-50 degrees and fixed at the CMC level with a 4-0 nylon suture which goes thru the CMC joint- head of metacarpal-CMC other lip.(Fig 17)

Figure 17: Index finger is fixed at CMC level
The Extensor/s are sutured first. The EIP becomes the EPL and the EDC becomes the APL
The Metacarpal level attachment of the EIP is dissected off; this enables the EIP to act on the DIP as an extensor. (Fig 12)
The EDC is kept attached at the base of the PPx of the IF so that once the tendon is reattached it acts as the APL.
The First dorsal interosseous is attached next to the lateral band to become the new abductor – opponens complex.(Fig. 18)
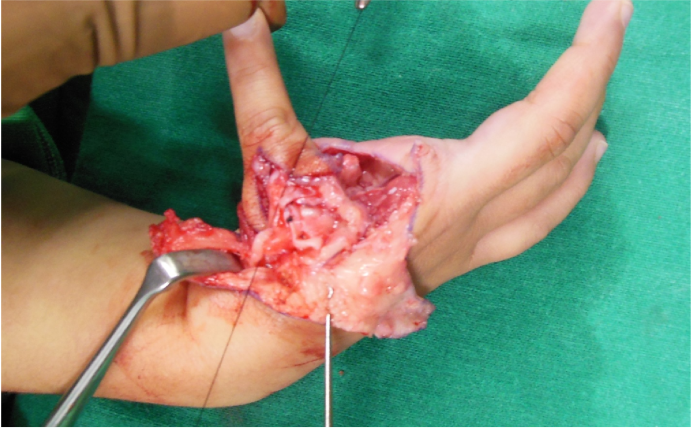
Figure 18: Suturing first dorsal interosseous to lateral band as the new abductor opponens complex
Dorsal flaps are sown.
The Palmar Interosseous is now attached to the other lateral band to become the Adductor Pollicis.
Skin flaps are now adjusted and closed to get the new thumb(Pollex) in opposition and pronation to achieve pulp to pulp pinch.(Fig. 19)
Fig. 20,21 show two views of the completed operation
 Figure 19: Adjusting skin flaps to get new thumb in opposition and pronation |
 Figure 20: Final position palmar view |
 Figure 21: Final position dorsal view |
A bulky padded dressing is given to protect the new thumb and tourniquet released and vascularity of both arteries and veins is checked.(Fig. 22)
Fig. 19 shows a long term result
 Figure 22: Final dressing |
 Figure 23: showing 7 years follow up results |
Complications of procedure
Losing the finger—very rare but possible
Skin necrosis
Hyperextension at CMC joint
Too long length
Functional Result may not be as good in severe radial longitudinal deficiency. There are chances of abnormalities of muscles of index finger and stiffness of index finger PIP joint in these cases (Symphalangism) which leads to relative functional impairment following pollicisation.
In our opinion it is still better than a four fingered hand at all times
Conclusion
Pollicisation is the optimum method of thumb reconstruction in thumb hypoplasia/aplasia
References
1. The rule of thumb by Tom Tyler JAC 30.3.4(2010) ,711-32.http://www.cyberchimp.co.uk/research/thumb.html
2. Lightdale-Miric N, Mueske NM, Lawrence EL, Loiselle J, Berggren J, Dayanidhi S, Stevanovic M, Valero-Cuevas FJ, Wren TA. Long term functional outcomes after early childhood pollicization. J Hand Ther. 2015 Apr-Jun;28(2):158-65
3. MahmutKömürcü, SerdarYüce et al. Index finger pollicization for treating a congenitally nonfunctioning thumb in patients with radial longitudinal deficiency. Eastern Journal of Medicine 2014;19: 175-181.
4. Tay SC, Moran SL, Shin AY, Cooney WC III. The hypoplastic thumb. J Am AcadOrthopSurg 2006;14: 354 –366.
5. Thumb hypoplasia .Scott A. Riley,Ronald C. Burgess. Hand Surg 2009;34A: 1564–1573.
6. James MA, McCarroll HR Jr, Manske PR. Characteristics of patients with hypoplastic thumbs. J Hand Surg 1996;21A: 104–113.
7. Abdel-Ghani B, Amro S. Characteristics of patients with hypoplastic thumb: a prospective study of 51 patients with the results of surgical treatment. J PediatrOrthop B 2004;13:127–138.
8. James MA, Green HD, McCarroll HR Jr, Manske PR. The association of radial deficiency with thumb hypoplasia. J Bone Joint Surg 2004;86A: 2196–2205.
9. Tickle C. Experimental embryology as applied to the upper limb. J Hand Surg 1987;12B: 294 –300.
10. Kato H, Ogino T, Minami A, Oshio I. Experimental study of radial ray deficiency. J Hand Surg 1990;15B:470–476.
11. Kozin SH. Deformities of the Thumb. Green’s Operative Hand Surgery.6 thed.ScottW.Wolfe, Robert N., William C., Scott K. editors. Philadelphia: Churchill Livingstone, Elsevier: 2011.p 1371.
12. Riley SA. An overview of radial longitudinal deficiency. CurrOrthop Prac2008;9:655–659.
13. Joseph Upton III and Amir Taghinia. Congenital hand III: Disorders of formation- thumb hypoplasia.James Chang and Peter C. Neliganeditors.Plastic Surgery- Hand and Upper Extremity.Elsevier Saunders,2013.p 572-602.
14. Gosset I: La pollicisation de I ‘index . J Chir.1949;65:403.
15. Bhaskaranand Kumar, Ashwath Acharya, and Anil K. Bhat. A relook at pollicization. Indian J Plast Surg. 2011 MayAug;44(2): 266–275.
16. Paul Binhammer and Graham Lister.Pollicization. Reconstructive Surgery in Hand Mutilation. Edited by Guy Foucher, Martin Dunitz: 1997.pg 29-40.
17. J W Littler, The neurovascular pedicle method of digital transposition for reconstruction of the thumb. Plast. Reconstr. Surg. 1953, 12:303-14
18. BuckGramcko D. Pollicization of the index finger. Method and results in aplasia and hypoplasia of the thumb. J Bone Joint Surg Am 1971;53:1605-17.
19. Yves Allieu, Michel Chammas and Jean Luc Roux. Considertions concerning pollicization. Reconstructive Surgery in Hand Mutilation. Edited by Guy Foucher, Martin Dunitz: 1997.pg41-52.
20. Thatte MR, Nehete S, Garude K, Mehta R. Unfavourable results in pollicisation. Indian J Plast Surg. 2013 May;46(2):303-11..
| How to Cite this Article: Hiremath AS, Raut BN, Yadav AA, Thatte MR. Pollicisation: Embryology, History, Technique and Results. International Journal of Paediatric Orthopaedics May-Aug 2016;2(2):29-33. |

Dr Mukund R. Thatte

