
Radial Hemimelia Treatment – Decision Making and Management, Algorithm of Management, Operative Approaches, Results
Volume 2 | Issue 2 | May-Aug 2016 | Page 17-23| Rujuta Mehta
Authors : Rujuta Mehta [1]
[1 ] HOD .Dept of Paediatric Orthopaedics. B J Wadia hospital for Children, Parel, Mumbai
[2] Dept of Paediatric Orthopaedics, Nanavati Superspeciality Hospital, Mumbai, India.
Address of Correspondence
Dr Rujuta Mehta
HOD, Dept. of Paediatric Orthopaedics, B J Wadia Hospital,
Nanavati Hospital, Jaslok Hospital & Shushrusha Hospital.
Email: rujutabos@gmail.com
Abstract
Radial hemimelia treatment has evolved a lot with many different types of surgical options; manifestations are myriad and presentations ages may vary from infancy to late childhood in most countries. A stepwise approach is needed for decision making and to manage this complex anomaly. The reader is presented here with a detailed clinical examination, decision making algorithm and an overview of surgical treatment options and the method preferred by the author with trends of interim and long term results and some other details in this review article.
Keywords: radial hemimelia, management, radial club hand
Introduction
Treatment for radial hemimelia has to be planned with a holistic picture in mind. The aim is to realign the carpus over the ulna in order to substitute for the missing radial pillar, as well as retain a good function, albeit without recurrence in an ideal world. The secondary issues of thumb aplasia and digital anomalies which invariably accompany the forearm deformity, need to be addressed separately: each on their own merit and severity. But since this anomaly involves multiple problems the whole balancing act is one of correct decision making and optimal clinical timing of each procedure.
Clinical examination
The first foundation for a proper decision making is a good clinical examination. The following typical features (as shown in Fig (1 and b) are often present and should be evaluated in detail

Figure 1 a: volar view of a radial club hand showing manus varus, severely bowed and shortened forearm ,mild thumb hypoplasia and symphallangic index and camptodactylous middle digits.

Figure 1 b: dorsal view of the same showing some amount of elbow hypoplasia clinically by lack of dimpling and flexion at the cubital fossa region, extremely short forearm and a pronounced volar subluxation at the wrist due to complete absence of the radial pillar
a) Mannus varus deformity of wrist
b) Shortened and or bowed forearm
c) With or without elbow synostosis or varying degrees of stiffness,
d) Thumb hypoplasia to aplasia,
e) Anomalies of the digits like symphallangism or camptodactyly,
f) Oligo dactyly or oligo-syndactyly.
The shoulder, elbow, wrist, and digital range of movement should be noted; in an infant often difficult; for active and passive motion. The ability to flex the elbow for hand-to-mouth function is examined, as this influences the treatment algorithm. Any procedure on the wrist is contra-indicated in the presence of an elbow synostosis. The position of the wrist with respect to the ulna and the ability to passively correct the radial deviation also are measured. The hand forearm angle (Fig 3a). as described by Manske and Goldfarb [1] should be carefully documented. The amount of ulnar bowing and angle of deviation from long axis should also be measured
The thumb is examined for hypoplasia and graded accordingly (elaborated in forthcoming part II of the symposium) Thumb deficiency contributes to functional impairment. Stiffness of the fingers is assessed, and the ability to grasp and release is determined via functional tasks. ‘Chop-stick ‘ grip between the index and middle finger or at times rarely even between ring and little finger is seen in late untreated children especially after 2 years of age . However the above features may vary with the degree of radial deficiency and the presence of associated anomalies. [2]. A thorough systemic evaluation is nevertheless mandated despite variations. The principal organ systems involved in these are the cardiac, renal, and hematological (though some of these may not manifest before 5 to 6 years of age), vertebral, occasionally foot and ankle, trachea-esophageal, and anal problems. Details of the various syndromes and their clinical relevance are explained in article by Chatterjee et al
Surgical Decision making
Type I radial club-hands have minor radial deviation of the wrist, which creates less of a functional problem than types II, III, and IV. (for details of classification refer to article by Sheth and Kumar) In these severe grades of dysplasia particularly with considerable absence of the radius, the wrist assumes severe radial deviation that increases to 90° over time. This further compromises the flexor and extensor tendons range and length, creating functional difficulty. The goals of treatment besides improving function of the extremity are [3,4] :
• To correct radial deviation
• Balance the wrist on the forearm
• Maintain mobility
• Promote growth of the forearm
• Enhance limb appearance for better body image
Centralization is indicated in radial club-hand types II, III, and IV, in which there is severe radial wrist deviation (than 30 degrees or more) [5] and insufficient support of the carpus. The carpal ring is pivoted back into position over the carpus by releasing all tethers on radial aspect, open reduction of ulno –carpal joint and capsulorrhaphy and restoring wrist stability, which is highly essential for development of a good power grip and other reconstructions. This is quite similar to what is done in developmental dysplasia of the hip. The optimum timing for performing centralization surgery is ideally 6 months of age before the onset of hand to mouth reflex. [8]. Correction of deformity early allows the brain cells to recognize normalized wrist alignment and mechanics as part of body image in the developing brain a phenomenon known as cortical adaption.
Thumb hypoplasia also requires consideration when formulating a treatment plan for radial club-hand. An absent or deficient thumb inhibits use of the hand in the correct prehensile way that was designed for human anatomy. Thumb reconstruction is usually delayed until after forearm treatment. Individuals not treated thus in the correct sequence of forearm and thumb correction may develop erroneous compensatory patterns like “chopsitick” action shown in (Fig 2b) which are very difficult to eliminate after early childhood as they get permanently established in the brain .
 Figure 2 a: Adult with untreated bilateral radial hemimelia. |
 Figure 2 b: same adult patient demonstrating chopstick action between index and middle finger. |
Contra-Indications
Contraindications for surgical intervention are a limited life expectancy in a child and elbow extension contractures that prevent the hand from reaching the mouth if the deformity at the wrist is corrected [6]. Surgery is also contraindicated for adults who have adjusted to their deformity (Fig 2a).
Investigations
As a protocol ALL radial dysplasia patients should be fully investigated and referred to pediatric subspecialists [2]. The heart is evaluated by auscultation and echocardiography. The kidneys are examined by ultrasound, and the platelet status is assessed by blood count and peripheral blood smear.
Plain radiographs are obtained to evaluate the degree of radial aplasia (Fig 3a) and to assess associated abnormalities of the elbow, wrist, and hand and spine when indicated . In radial club-hand, ossification is delayed,(fig 3b) and final determination of complete aplasia of the radius or carpus must be deferred until later almost up to the age of 8 years ( Fig 3c). In some cases a frank synostosis of the ulno- humeral joint may also be seen early. X rays of the whole spine AP and lateral should also be done as a screening to detect subtle VATER anomalies and vertebral involvement. In established cases it is better to evaluate the spinal involvement with more focused and detailed x rays and higher imaging whenever necessary.
For details of further investigations particularly the hematological ones which may have a bearing on the life expectancy of the child please refer to chapter no 2. The visceral anomalies get priority over centralization if life threatening , but with modern day anesthesia techniques of regional anaesthesia even high risk cases can be operated maybe a few months later than expected but within infancy period.
 Figure 3 a: Hand forearm angle .the angle between the line D : which is the line connecting the midpoint of the transverse axis of the ulna with the midpoint of the transverse axis of the 3rd metacarpal base which has to be parallel to the long axis of the distal ulna. The angle B is then formed between the long axis of the 3 rd metacarpal and the perpendicular joining the midpoint where the line D ends. |
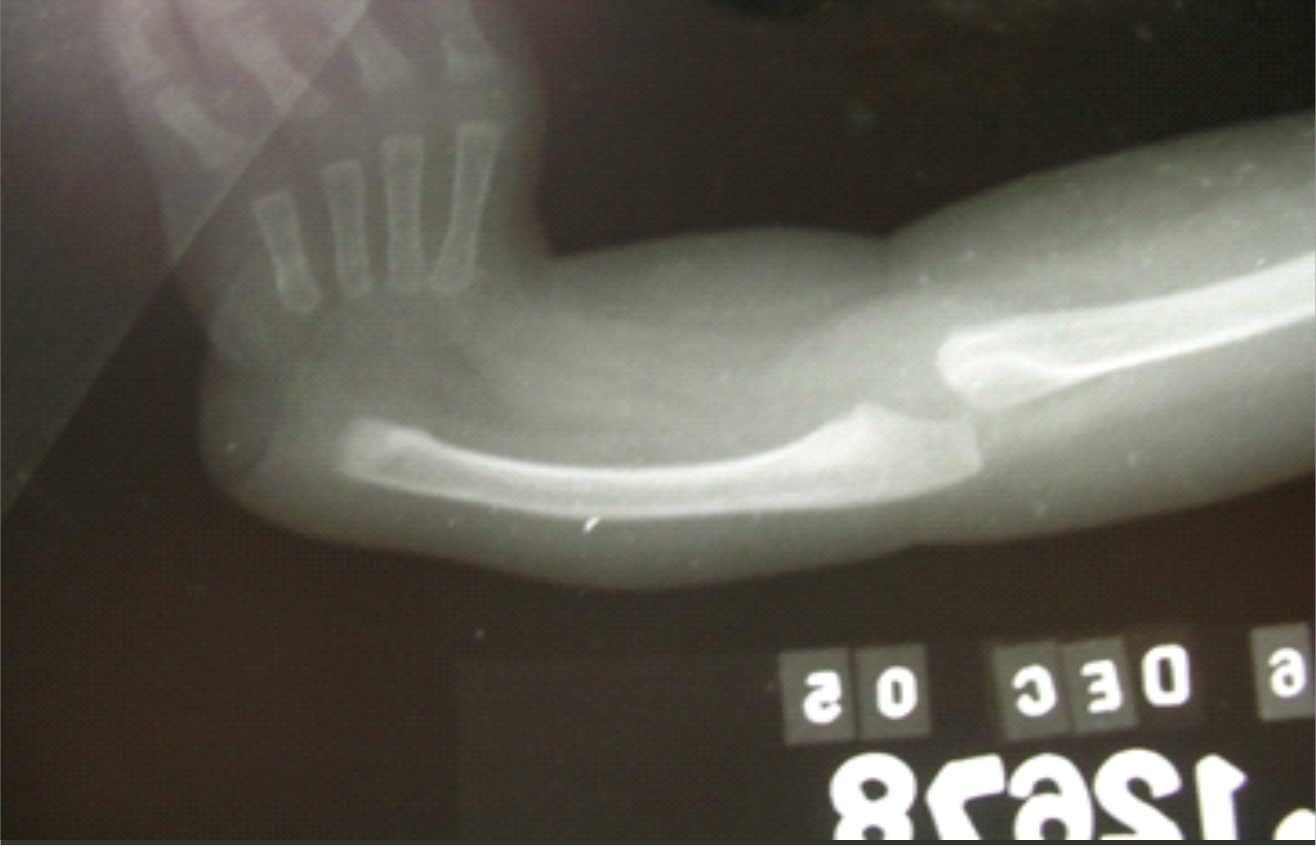 Figure 3 b: X ray of a radial club hand at 4 months of age showing seemingly complete absence of radius and a very light cartilaginous shadow of the anlage . |
 Figure 3 c: x ray of the same child shown in fig 3 a, at 8 years of age showing good ossification of radius changing the grade of classification. |
Surgical Treatment
Correction of radial club hand especially the more severe grades (which are incidentally commoner) requires a combination of non-operative and operative management that begins shortly after birth.
Early ( 0 to 3 months of age )
Treatment begins with counseling about nature and prognosis, when the child presents at birth to ensure a less drop- out rate and eradication of emotional and social stigma. Passive stretching of the taut radial structures is started at the initial visit. Stretching is performed at each diaper change and at bedtime. A stiff elbow with limited motion also is stretched during this time. Splint fabrication should be done with heat mouldable materials .Serial plasters are challenging until 3 months of age due to the extremely short working length of the forearm. When started at around 3 to 4 months of age however are certainly beneficial in maintain the suppleness and preventing wound complications post op.
Soft tissue distraction techniques [7], various fixator –distractor assemblies have been used with great enthusiasm for primary distraction both for late cases [13] and early in severe deformities. The author also prefers to use distraction with the mini ex fix for gr 3 and 4 radial club hands with angulation over 450. The principles, technique and results of the same have been highlighted in chapter [6].
Operative Methods
Early intervention takes advantage of the ability of the immature brain to adjust. Children with bilateral deficiencies that affect both the forearm and thumb require staged treatment to gain maximal use of the reconstructed limbs. Centralization of the wrist on the ulna to date remains a popular treatment to correct radial deviation. This procedure is performed in patients aged ideally 6 months of age before the onset of hand to mouth reflex vide Buck Gramko [8]. Surgery at this time allows for improvement in forearm length and provides a foundation for the development of motor function within the hand and for better cortical adaption in the growing immature brain.
Buck –Gramko [ 8] in his classical technique of Radialisation improved the ulnar lever arm by transferring the radial flexor and extensor to the ulnar aspect reversing the imbalance of the tight and strong radial musculo-tendinous units; which gained wide acceptance. This technique of tendon transfer is applicable and adequate to treat, grade 1 and 2 radial hemimelia cases where the deforming forces need to be converted to corrective forces in order to restore soft tissue balance at the wrist (Fig 4 a, b,c,d,e) . In an ideal world all radial club hands thus treated would not recur –but very often one encounters missing or short tendons especially in grade 3 and 4 radial dysplasia, and hence not available or adequate for a perfect rebalancing the deforming forces. As a pioneer in this field Prof. Buck Gramko also showed that excision of carpal bones and ulnar epiphyseal cartilage for grade 3 and 4 radial club hands ; is not only unnecessary, but its preservation leads to better range of wrist motion post surgery
 Figure 4 a: X ray of Gr 2 radial club hand. |
 Figure 4 b: FCR identification for tendon transfer volar aspect grade 2 radial club hand. |
 Figure 4 c: ECR identification on dorsal aspect grade 2 radial club hand. |
 Figure 4 d: ECU identification on volar aspect in grade 2 radial club hand. |
 Figure 4 e: result after tendon transfer in grade 2 radial club hand showing complete correction. |
Surgical Approaches
The skin incision and approach for open surgery has varied from author to author. Buck-Gramcko [8] and Lamb [3] favored the dorsal lazy S shaped approach (Fig 5a) this incision is not very aesthetic and runs opposite to the lines of langer and natural healing. Hence if there a wound dehiscence or hypertrophy it becomes a very unsightly scar .The disadvantages being a lack of radial skin in late and severe deformities and redundancy of the ulnar skin after correction, which needs unnecessary excision of good skin. Others have recommended a Z plasty (Fig 5b) along the concave radial border, and adding a longitudinal incision along the ulnar border overlying the ulno-carpal joint; the skin bridge between the two incisions however impedes access. Manske [1] used a single ulnar transverse ellipse incision (Fig. 5c) and so did Flatt but invariably both methods have been unable to solve the problem of unnecessary excision of ulnar skin.
 Figure 5 a: dorsal incision as described by buck Gramcko |
 Figure 5 b: Z plasty incision radial aspect. |
 Figure 5 c: manske incision ulnar transverse ellipse. |
Evans [9] in 1995 published his bilobed flap .He and his co authors have described a bilobed incision in which skin from the dorsum of the hand is transposed to the radial side to cater to the shortage, and the redundant excess is utilised to cover the defect now created on the dorsum.(Fig 6a,b).
 Figure 6 a: Bilobed flaps raised , note forceps pointing over the ulnar redundancy flap. |
 Figure 6 b: Bilobed flaps moved , ulnar flap moved into dorsal and dorsal moved into radial defect , note forcep is pointing to the ulnar defect which closes by primary intention. |
There is a significant learning curve associated with this flap. In experienced hands the incision may heal as beautifully as shown in fig (Fig 6c, d) and may not even be seen if covered with a bracelet or watch or shirt sleeve (Fig 6e,f)
 Figure 6 c: Ulna flap perforator marked by arrow. |
 Figure 6 d: closure of moved dorsal flap over radial defect. |
 Figure 6 e: closure of moved ulna flap over dorsal defect. |
 Figure 6 f: healing of moved dorsal flap. |

Figure 6 g: healing of dorsal flap and ulna defect.
This too is fraught with a pitfall of superficial necrosis if the adipo-venous plane is violated. (Fig 7 a,b) The trick however is to keep the flap harvest as glabrous as possible taking care to maintain the perforator vessel feeding the flap as shown in (Fig 6c) and not skeletonising the ulna head as otherwise it may contribute towards physeal growth arrest of distal ulna [10]. The final closure too must be without tension. The advantages of the overall 360 degree exposure of the upper end ulna and carpus achieved with this flap and the ease of reduction, far outweigh its disadvantages, which can be easily managed with conservative treatment.
Pilz murdin [11] compared the 5 diffirent incisions described above .according to them the preferred practice in each region has by and large varied a lot however , now the bilobed flap is gaining popularity . The author personally prefers to have the best of both worlds , i.e. combine the advantages of distraction with a good surgical exposure and aesthetics and hence has been practicing the below highlighted method since almost 17 years now the mid term results of which are already published [16]
 Figure 7 a: superficial to moderate necrosis of dorsally moved ulna flap. |
 Figure 7 b: superficial necrosis of moved dorsal flap over radial defect |
Pre-Operative protocol
The main preoperative emphasis is placed on the status of soft tissues. Stretching and splinting of the taut radial structures is required prior to surgery. Failure to elongate the tight radial side limits the ability to centralize the wrist on the ulna. Preliminary soft-tissue lengthening with an external fixator is a option in cases recalcitrant to stretching, such as in older children or patients with a recurrent deformity.[7, 16]
Preoperative measurements of the degree of active and passive motion of the digits and wrist are recorded. Radiographs in the anteroposterior and lateral projection, including the elbow and hand, are obtained. The degree of ulnar bow is calculated from the lateral radiograph as the angle between the proximal and distal ulna. Angulation of more than 45° usually requires corrective ulnar osteotomy at the time of centralization to realign the forearm. Some authors however delay the ulna osteotomy as a second stage. This too is well accepted and is a prerequisite before limb lengthening .The sites, method and technique with fixation of ulnar osteotomy and results have been eluded to in detail in part II of the symposia
Surgical technique /Essential Steps
1. Incision and exposure of radial side defect with incision and approach. The author is well versed with the bilobed Evan’s flap (Fig 8) for grade 4and prefers to use the same in majority of cases. for grades 2 and 3 where a significant amount of dissection is required on the ulnar side, the author prefers the Manske ulnar approach (Fig 5 c) .For grade 1 and 2 radial club –hands where the skin shortage is not there and hence rebalancing is not required; the author usually uses bilateral Z plasties if the skin is tight or the Manske approach coupled with a mirrored radial transverse half incision like a hemi cincinnati incision used in club feet.
2. Identification of median nerve which may be tented over the defect and retraction out of harm’s way.
3. Identification and isolation of flexor carpi radialis along with the muscle belly and harvest over a stay suture :(if present) or hypoplastic and short especially where the thumb is well developed and the grade of dysplasia is mild.
4. Identification of extensor carpi radialis along with muscle belly and freeing its excursion by releasing the tight sheaths (differentiation of longus and brevis or two slips maybe deficient), and harvest over a stay suture.
5. Identification and excision of radial anlage, freeing the carpus from underlying fibrotic tissue.
6. Mobilizing the carpus to open up the radial side soft tissue upto neutral.
7. Proceeding with identification of extensor carpi ulnaris which is usually thick, redundant and curved over the head of the ulna and retracting it away.
8. Identification of the flexor carpi ulnaris which may be short and stubby but hypertrophied.
9. Open reduction of wrist joint at the cleavage of ulno-carpal junction by a sharp dissection. The recognition of this plane is aided either by a sharp needle or with performing wrist dorsiflexion and palmar flexion.
10. Passing a kirshner wire retrograde through the 2nd metacarpal and then back into the carpus after moving the carpus ulnar ward, to centre the wrist over 2nd metacarpal base where possible. Some authors resort to creating a notch in the carpal bed and the tapering edge of ulna to fit the mismatched sizes into each other. This was practiced and probably still is by a large section of orthopaedic surgeons still doing a single stage procedure in late and difficult cases. The argument for this being that the stability that this affords to the reduction is very much needed for preventing recurrence. However long term studies on ulna growth patterns have shown that this further reduces the growth potential of the hypoplastic limb.
The author strongly advices against the notch plasty and personally prefers to use pre-op distraction to aid with the reduction and preserve the growing cartilage at the wrist.
11. Careful reefing of the wrist joint capsule, particularly over the dorsal carpal area, and double breasting where required to prevent future volar subluxation. Do not proceed with the completion of tendon transfer unless wrist capsule closure is secured.
12. Completion of tendon transfer of flexor carpi radialis to flexor carpi ulnaris on volar aspect, and extensor carpi radialis to extensor carpi ulnaris dorsally. If the tendons falls short periosteal sleeves form the base of the metacarpals may be used or simple the tethering force on radial side may be released ad attached as ulnar ward as possible.
13. Skin and soft tissue closure without tension and above elbow slab over a well double padded dressing.

Figure 8: Direction of flap movement , B transposes with rotation to A, and A transposes to radial defect.
Post Operative Protocol
Immediate active and passive digital motion is initiated, along with measures to reduce swelling. The timing of K-wire removal is largely need based. At least 6 to 8 weeks of fixation is desirable till the carpus stabilizes. Some authors however recommend 12 weeks prior to removal; in practical terms it is usually difficult to maintain for this long and may invite complications like loosening and infection. Following K-wire extraction, a splint is made and removed for exercises, with gradual weaning from the splint over the next 4-6 weeks. A night-time splint regimen is encouraged until skeletal maturity is reached.
At some centers the tendon and/or bony procedures are performed simultaneously to better align the forearm and to balance the wrist. The extensor carpi ulnaris is used to increase its moment arm for ulnar deviation. Other less common options are discussed in part II of the symposia. Unfortunately, no method reliably and permanently corrects the radial deviation, balances the wrist, and allows continued growth of the forearm [12, 13]. Recurrence ,complications and long term problems are discussed in part II of the symposia. The maintenance of the carpus at the end of the ulna without sacrificing wrist mobility or stunting forearm growth remains a daunting task.[12, 13]
Follow-up and Results
Patients with radial deficiencies require follow-up into adulthood. The evaluation should include not only the status of the centralization but also any additional operative and non-operative needs [14,15]. The shortened extremity with diminished motion may not be able to accomplish certain functions. These tasks often can be carried out with the use of assistive devices. In addition, as the child ages, distraction osteogenesis may be an option to increase forearm length. As this review is being published , the authors personal experience with results of long term follow up with solutions to tackle the bowstring effect causing residual radial deviation and especially volar re-subluxation with follow up results of ulna growth and breadth are being analysed . The trends show much higher percentage of ulna growth almost above 70% and the diameter hypertrophy is way beyond expectation (Fig 9 and 10). This goes to prove that the earlier the procedure is done, the realigned carpus remodels the ulna dome to form a stable receptacle and support. Thus the growing cartilage is retained and it adapts to the function of the missing radius well.
 Figure 9: Clinical mid term result. |
Complications are common following centralization and can occur at the time of surgery or during the post-operative or follow-up period. Intra-operatively damage to the median nerve should be meticulously avoided by the use of careful blunt dissection and magnification loops during the surgery. The most important complication is compartment syndrome in the initial post op period and must be guarded against, by avoiding water tight skin closure, using loose well-padded dressing. Most other complications with our technique are minor and do not impact the overall outcome. These include pin-tract irritation and a transient diminution in finger motion. When using the distraction techniques instances of physeal distraction have been reported. These can be managed by immediate removal of fixator and immobilization in POP cast.
Recurrence is the most common source of failure after operative treatment, and the cause appears to be multi-factorial. Operative causes of failure include the inability to obtain complete correction at surgery, inadequate radial soft-tissue release, and failure to balance the radial deforming force, early k wire removal, poor postoperative splint use, and the natural tendency of the shortened forearm and hand to deviate as a natural consequence of the bow string effect of the long flexor tendons.
The application of sophisticated techniques, such as distraction osteogenesis and microsurgery [13], to the treatment of radial club-hand introduces additional potential complications, such as fracture of the regenerate bone, digital stiffness from lengthening, and vascular thrombosis of the microsurgical anastomosis.

Chart 1: Algorithm for Management as per grade of Hemimelia
References
1. Manske PR, McCarroll HR Jr, Swanson K. Centralization of the radial club hand: an ulnar surgical approach. J Hand Surg [Am]. Sep 1981;6(5):423-33.
2. Goldfarb CA, Wall L, Manske PR. Radial longitudinal deficiency: the incidence of associated medical and musculoskeletal conditions. J Hand Surg [Am]. Sep 2006;31(7):1176-82.
3. Lamb DW. Radial club hand. A continuing study of sixty-eight patients with one hundred and seventeen club hands. J Bone Joint Surg Am. Jan 1977;59(1):1-3. [
4. Goldfarb CA, Klepps SJ, Dailey LA, Manske PR. Functional outcome after centralization for radius dysplasia. J Hand Surg Am. 2002 Jan;27(1):118-24
5. McCarroll HR. Congenital anomalies: a 25-year overview. J Hand Surg [Am]. Nov 2000;25(6):1007-37.
6. Bayne LG, Klug MS. Long-term review of the surgical treatment of radial deficiencies. J Hand Surg [Am]. Mar 1987;12(2):169-79.
7. Nanchahal J, Tonkin MA (1996). Pre-operative distraction lengthening for radial longitudinal deficiency. Journal of Hand Surg [Br] 21:103-7.
8. Buck-Gramcko D. Radialization as a new treatment for radial club hand. J Hand Surg [Am]. Nov 1985;10(6 Pt 2):964-8.
9. Evans DM, Gately DR, and Lewis JS.The use of bilobed flap in the correction of Radial Club Hand .Journal of Hand surgery, 1995; 20B:333-337,
10. Heikel HV. Aplasia and hypoplasia of the radius: studies on 64 cases and on epiphyseal transplantation in rabbits with the imitated defect. Acta Orthop Scand Suppl. 1959;39:1-155.
11. Pilz SM, Muradin MS, Van der Meule JJ, Hovius SE. Evaluation of five different incisions for correction of radial dysplasia. Journal of Hand Surg 1998;23B:183-5.
12. Sestero AM, Van Heest A, Agel J. Ulnar growth patterns in radial longitudinal deficiency. J Hand Surg[Am]. Jul-Aug 2006;31(6):960-7.
13. Vilkki SK. Distraction and microvascular epiphysis transfer for radial club hand. J Hand Surg [Br]. Aug 1998; 23(4):445-52.
14. Damore E, Kozin SH, Thoder JJ, et al. The recurrence of deformity after surgical centralization for radial clubhand. J Hand Surg [Am]. Jul 2000; 25(4):745-51.
15. Kozin SH. Upper-extremity congenital anomalies. J Bone Joint Surg Am. Aug 2003; 85-A (8):1564-76.
16. Thatte MR, Mehta R. Treatment of radial dysplasia by a combination of distraction, radialisation and a bilobed flap – the results at 5-year follow-up. J Hand Surg Eur Vol. 2008 Oct;33(5):616-21.
| How to Cite this Article: Mehta R. Radial Hemimelia Treatment – Decision Making and Management, Algorithm Of Management, Operative Approaches, Results. International Journal of Paediatric Orthopaedics May-Aug 2016;2(2):17-23. |

Dr. Rujuta Mehta

