Percutaneous centralization for Radial Club Hand – A Technical Note
Volume 2 | Issue 3 | Sep-Dec 2016 | Page 19-23 | Sandeep Patwardhan, Kunal Aneja, Ashok Shyam
Authors : Sandeep Patwardhan [1] , Dr Kunal Aneja [1], Ashok Shyam [1]
[1] Sancheti Instittue for orthopaedics and Rehabilitation, Pune, India.
[2] Indian Orthopaedic Research Group, Thane, India.
Address of Correspondence
Dr Sandeep Patwardhan
Sancheti Instittue for orthopaedics and Rehabilitation, Pune, India
Email: sandappa@gmail.com
Abstract
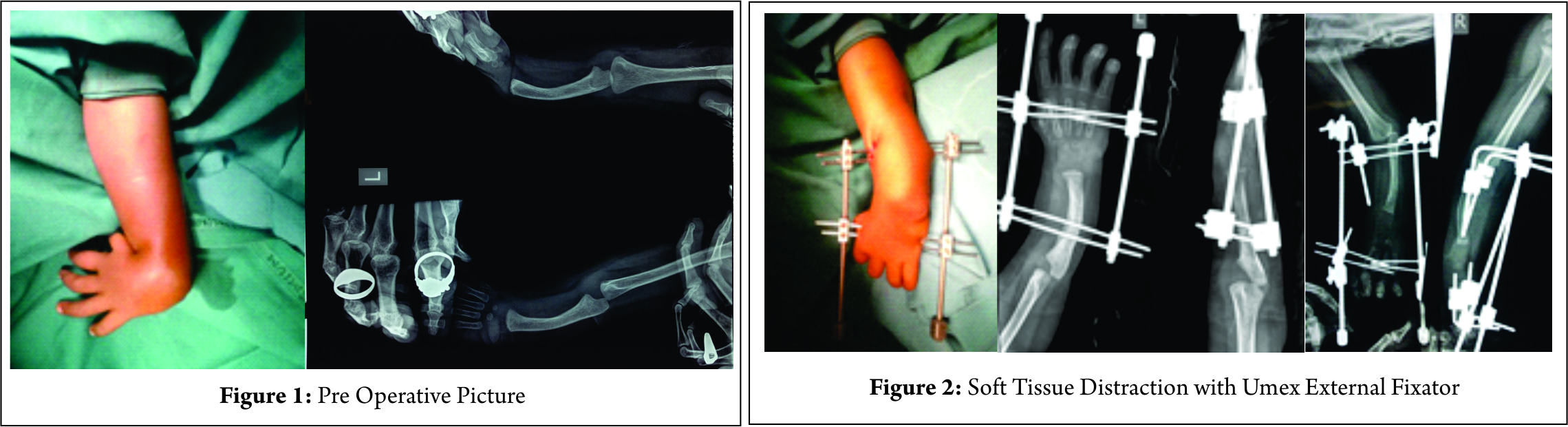
The treatment for radial club hand (Heikel Type III and IV) in stages of soft tissue distraction, followed by centralization of carpus over ulna and later pollicisation has been reported. Traditionally the described procedure for centralization of the carpus over the ulna has been by an open approach, involving placing the growing inferior end of ulna over center of carpus and maintaining it with a K wire. Open centralization procedure is fraught with dangers of damage to cartilage, scarring and stiffness of wrist joint, thus increasing morbidity of the procedure. We describe a new technique of percutaneous closed centralization, taking advantage of pliability of soft tissues achieved by distraction method, thus preserving the biology and function. This technique, to our knowledge, has not been reported earlier and we have found it to be a simple and effective method to achieve centralization for patients with radial club hand.
Keywords: Radial club hand, percutaneous centralisation, ulna osteotomy.
Introduction
Radial club hand is a relatively rare deformity with an incidence of 0.5 per 10,000 live births [1,2,3]. Petit was the first individual to record the first case of radial club hand in the year 1733[4]. Radial club hand is divided by Heikel[5] into four types out of which Type III and IV are considered to be the most common forms[5]. These cases also tend to be associated with the greatest amount of radial deviation of the wrist. Over the years, the management of radial club hand has undergone significant changes. In severe cases (Heikel[5] Type III and IV), requiring surgical intervention for deformity correction and improvement of function, historically various surgical treatment modalities have been performed like ulnar osteotomy and splitting the distal ulna for insertion of the carpus [6], serial casting and open centralisation[7] , ilizarov correction[8,9], reconstruction by a bone graft and non-vascularized epiphyseal transfer[10],vascularized proximal fibular epiphyseal transfer[11]and pollicization[12,13].We believe, a staged treatment of radial club hand involving soft tissue differential distraction, percutaneous centralization and pollicization offers a biological solution to this complex problem, for deformity correction and to enhance function.
Procedure : Staged surgical correction of radial club hand deformity is done in the following manner-
Stage 1 : Soft tissue differential distraction
Done by Using a Universal Mini External Fixator (UMEX fixator) to slowly distract the soft tissues and correct the radial deviation. (Fig. 2 a, b)
1. Under suitable anesthesia and under all aseptic precautions, painting and draping of affected upper limb is done.
2. Two K wires of 1.5 mm diameter each are passed at mid metacarpal level, parallel to each other and passing through all the metacarpals in the coronal plane.
3. Two K wires of 2 mm diameter each are passed parallel to each other at the apex of ulnar bowing, again in the coronal plane.
4. These are connected across carpus using universal mini external fixator for soft tissue distraction, such that one connecting rod is towards the concave (radial) and the other towards the convex (ulnar) side of the deformity. It is usually possible to passively accommodate these K wires in same plane. In case it is not possible to do so, additional frame may be constructed so that the distractors are placed in a coplanar fashion. (Fig. 2c)
5. After 2nd post operative day, differential distraction is started which involves distracting at rate of 1mm/day on radial side in 4 graduated turns of 1/4th mm each and 0.5mm/day on ulnar side in 2 graduated turns of 1/4th mm each. This is taught to the child’s parents for them to continue at home.
6. Adequate pin tract care is taken with regular pin tract dressing on alternate days. Weekly X-rays are taken to confirm centralization of carpus over ulna and distraction across carpus.
7. The guided differential distraction is continued for 4 weeks till the radial deviation of hand is obliterated and the hand is visibly angled slightly to ulnar side.
8. After this is achieved, distraction is stopped and the external fixator is kept in static mode for additional one week, to allow for the soft tissues to stretch. This stretching of soft tissues allows for passive correction of deformity.
Thereafter, as a second stage procedure, external fixator is removed and percutaneous centralization of carpus over ulna is done.
On removal of external fixator frame, it is observed that soft tissue pliability achieved by distraction allows the hand to be placed in over corrected position in relation to ulna. (Fig. 3)
Stage 2: Percutaneous centralization:
1. Neutralizing the hand in relation to forearm, such that there is no visible deviation of hand in both coronal and sagittal planes. This involves holding the hand in line with the forearm in antero posterior view and also ensuring that there is no visible volar deviation of wrist in lateral view. (Fig. 3)
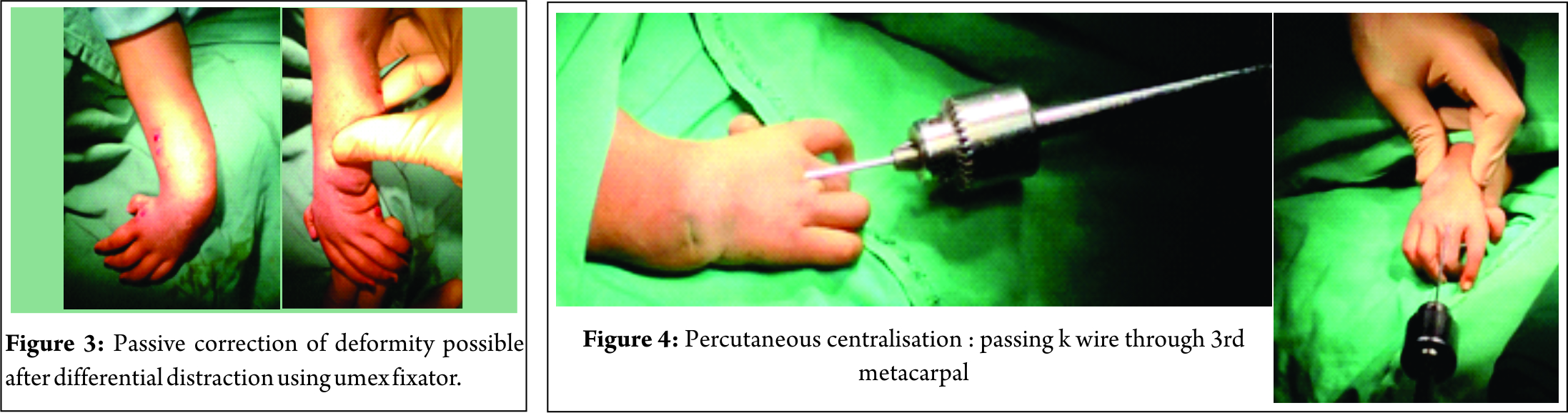
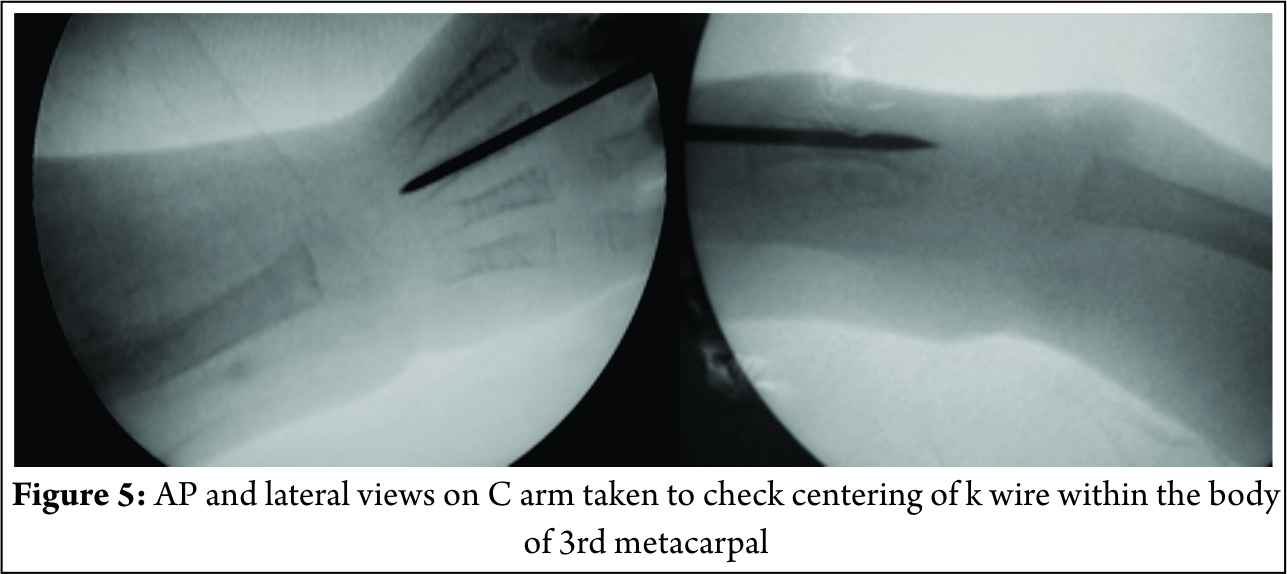
2. After flexing the metacarpals to 90 degrees, to make the head of 3rd metacarpal more prominent and moving the base of the proximal phalynx away, a 2mm K wire is loaded on Jacobs chuck T handle and is advanced in retrograde fashion from head of 3rd metacarpal. It is passed through the distal end of 3rd metacarpal, into its body and exited from its proximal end. (Fig. 4) The positioning of K wire within the substance of 3rd metacarpal is important and hence checked under image intensifier in both anteroposterior and lateral views. (Fig. 5)
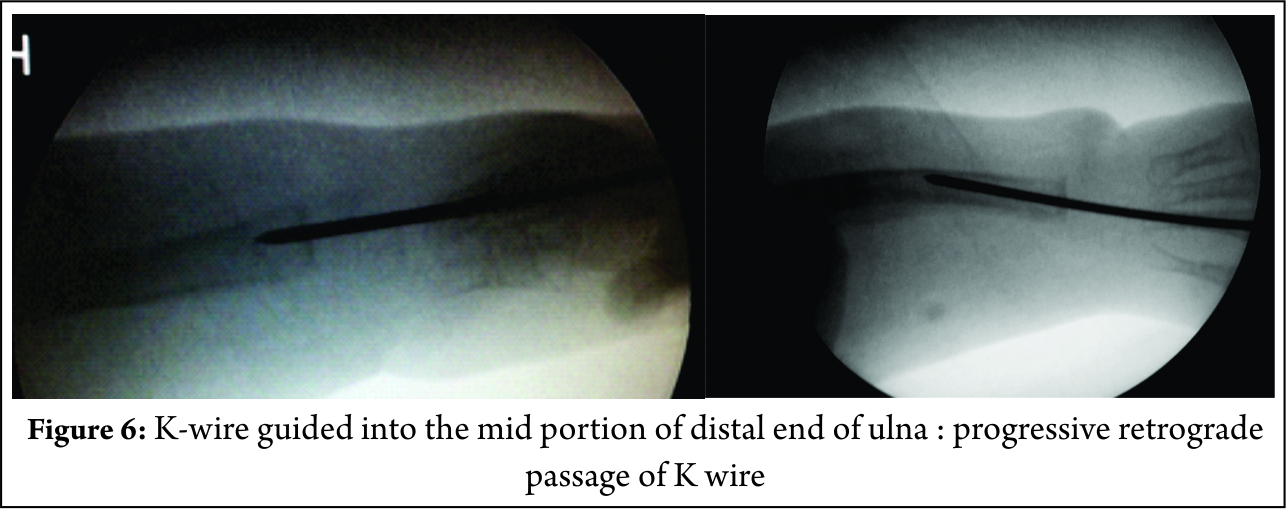
3. With manual traction and manipulation, K wire is then centralized over mid portion of distal end of ulnar epiphysis and progressed in a retrograde manner, under image intensifier guidance. The correct selection of entry point in ulna is important to maintain the hand in neutral corrected position in relation to the forearm. Checking it under antero-posterior and lateral views of C-arm ensures that the entry point is in the center of distal ulnar epiphysis. (Fig. 6)
4. In some cases, due to bowing of the ulnar shaft, K wire may hit the apex of ulnar deformity and hence may exit more distally (middle third) in the ulnar shaft. In such cases, to allow for the K wire to exit from proximal 1/3rd aspect of ulnar shaft, following methods can be used to straighten the ulna:
Closed plastic deformation of ulna (Fig. 7) : pressure is applied over the apex of the ulnar bow with the thumb and deformity is corrected under image intensifier guidance. K wire is then guided in a retrograde fashion into the straightened ulna. This K wire prevents the deformed ulna from regaining its original contour.

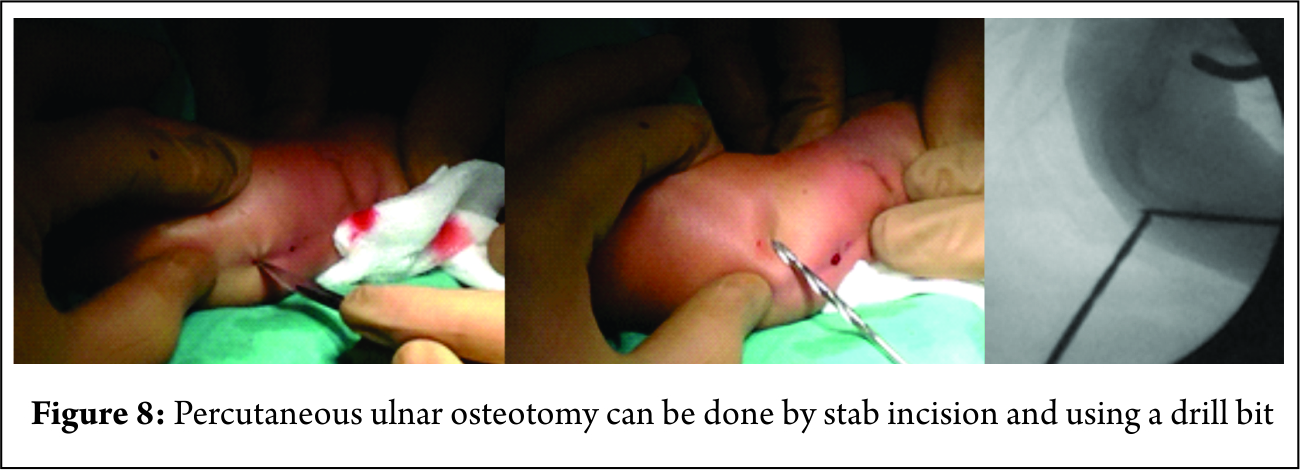
Percutaneous ulnar osteotomy (Fig 8) : If plastic deformation doesn’t help achieving a straightened ulna, ulnar osteotomy may be warranted. For this, a stab incision is taken over the apex of the ulnar bowing and percutaneous ulnar osteotomy is achieved by drilling with a drill bit. K wire is then guided into osteotomised ulna such that the coronal bowing is maximally corrected (Fig. 9)
Ideally the K wire should exit from the proximal third of ulnar shaft, as proximally as possible. In cases, where minimal bowing of ulna is there and apex of ulnar bowing lies in proximal 1/3rd of ulna, neither osteotomy nor plastic deformation is required and the ulna remodels as the patient grows.
5. K wire is then progressed further proximally through the ulna such that it exits from its proximal end, as proximally as possible. A small nick is made over the skin overlying the K wire, to expose the K wire.
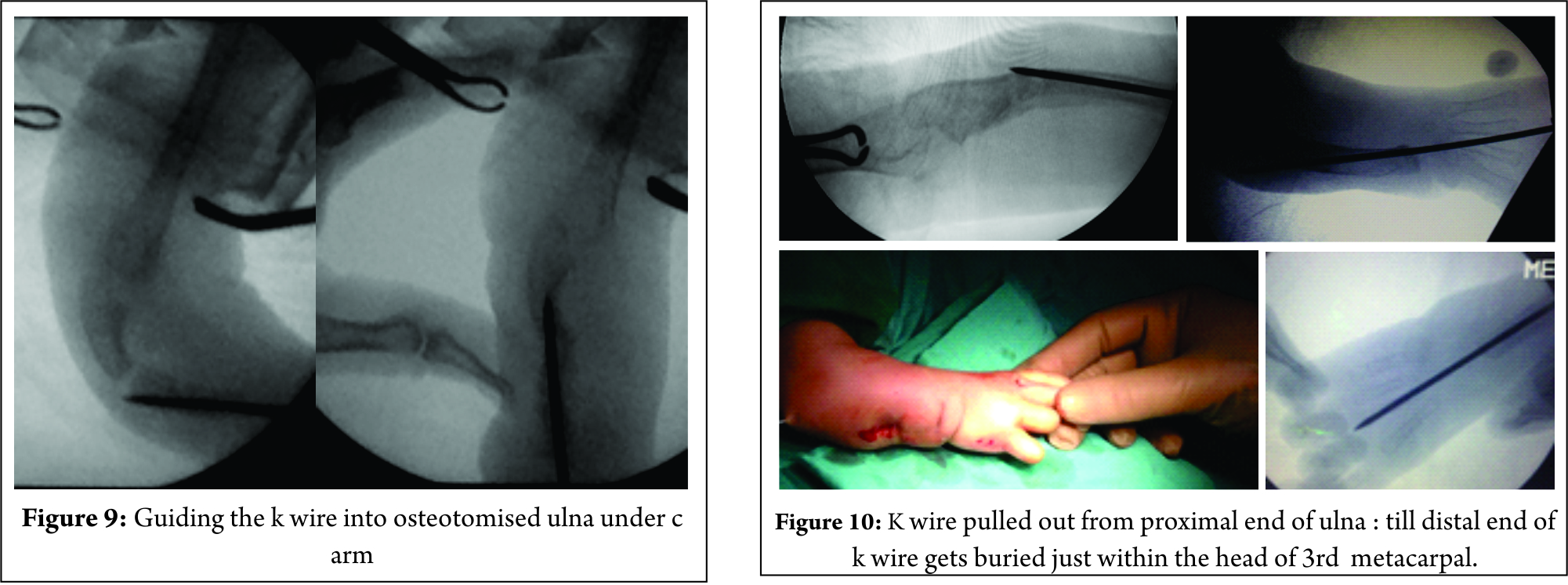
6. K wire is pulled out from the proximal end of ulna with a nose plier till its distal end gets completely buried just within the head of the 3rd metacarpal, to allow for free movements of 3rd Metacarpo-phalangeal (MCP) joint which is checked intra operatively. (Fig.10)
7. Excessive length of the k wire is cut off, bending and burying the remaining portion under the skin and closing the skin incisions primarily with ethilon sutures.
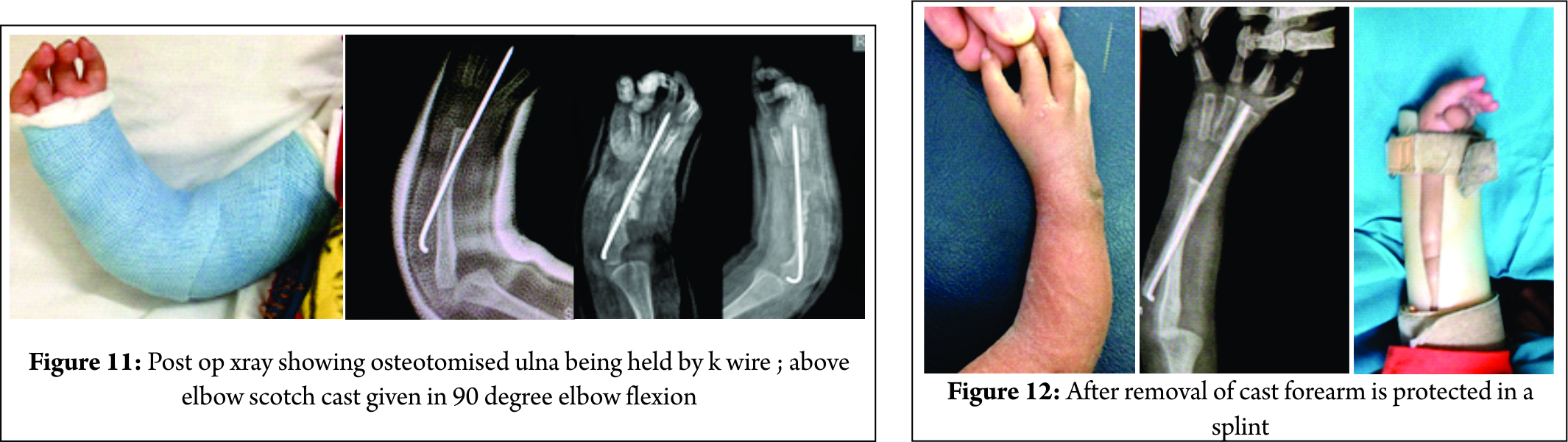
8. To immobilize and externally support the fixation, above elbow scotch cast is given in 90 degrees of elbow flexion for a period of 4 weeks. (FIG 11)
9. After a month, cast is removed and removable brace in the form of PVC ulnar gutter splint is given to support the wrist and forearm in neutral position. (FIG 12)
10. Active and passive range of motion exercises are encouraged for the elbow and fingers of the involved hand.
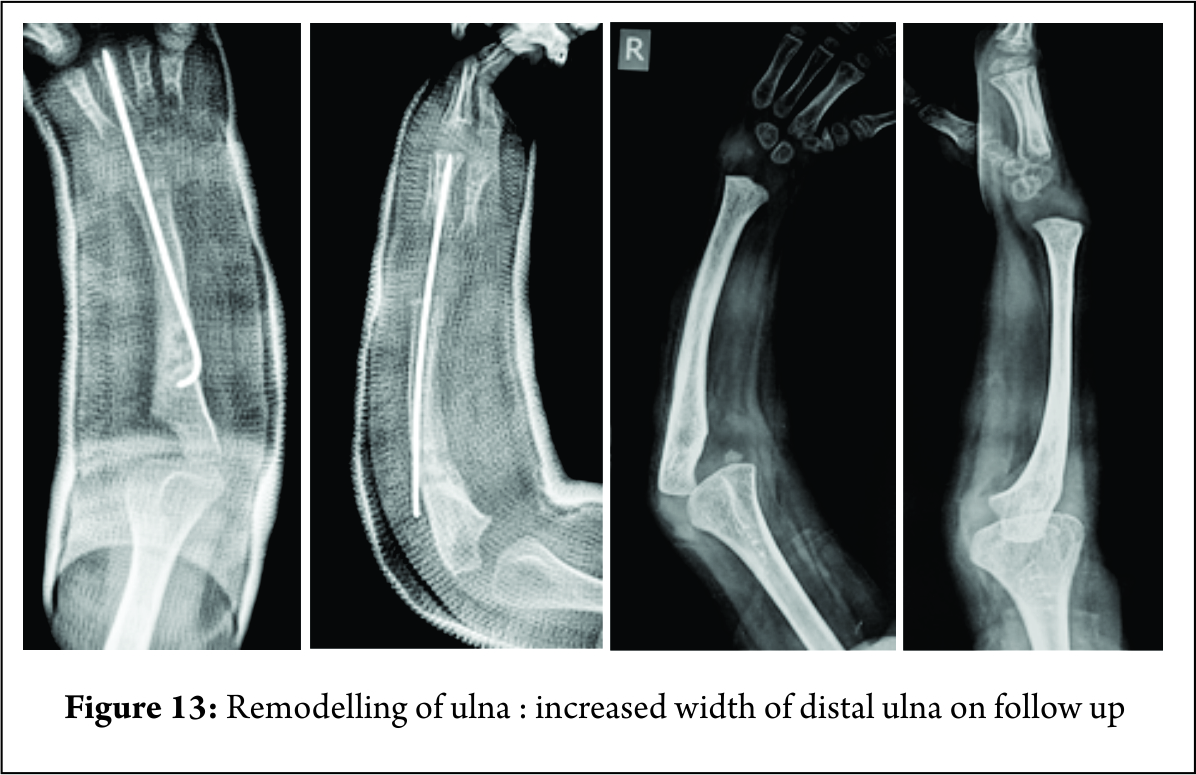
11. The K wire is kept in situ for maintaining the alignment of carpal bones over the ulna, till the distal ulnar epiphysis widens to accommodate the carpal bones. This distal ulnar remodeling is assessed with radiographs obtained on regular 3 monthly follow up visits. (Fig. 13) We believe this biological plasticity of distal ulna is better served by a closed procedure. K wire is retained in situ for an average period of 1.5 to 2 years, after which it is removed. Pollicisation is done 3 months after centralization procedure.
12. For K wire removal, under image intensifier guidance, a small skin incision is taken over the proximal end of ulna, in line with the intraosseous K wire, and blunt dissection is done to expose the proximal end of K-wire. In those cases where the wire becomes buried under bone due to cortical bone covering it, overlying bone is nibbled out and then the K wire is exposed. K wire is then removed by withdrawing it proximally through this incision. After removal, skin is primarily closed with ethilon sutures.
Discussion
The aim of this technical note is to introduce and describe an innovative technique of percutaneous centralization in staged treatment of patients diagnosed with radial club hand. Advantage of this technique is that it being a closed procedure, involves minimal soft tissue dissection, thus reducing the chances of growth plate injury and is easily reproducible after a short learning curve. The current treatment method followed, where centralization is achieved by an open technique, involves extensive soft tissue dissection and has been associated with high rates of physeal injury [14], recurrent radial deviation [15], and wrist stiffness [16]. Iatrogenic physeal injury can hamper the growth potential of the already shortened forearm and can increase the limb length discrepancy [14]. Complications of the technique described here can be infection leading to K Wire loosening and back out or bending of K wire, recurrence of deformity [15] and restricted wrist range of motion after K Wire removal. Since this staged treatment involves usage of an UMEX external fixator for soft tissue distraction prior to centralization, many parents might be apprehensive with the usage of an external fixator for 6 weeks duration, hence reducing the acceptability of this staged procedure. Many authors have described the usage of an external fixator for radial club hand correction previously. On the other hand, in those patients in whom the radial deviation of hand is passively correctable prior to the start of treatment, primary objective, which is to maintain neutral hand forearm position, can be achieved by directly percutaneously centralizing the hand without soft tissue distraction. A long term follow up study of a large sample size is required to establish the efficacy of this technique and document the complications associated with it.
Summary: The technique of percutaneous centralization of carpal bones over radius is recommended as part of a staged procedure, following soft tissue distraction with UMEX fixator. It is an innovative biological approach relying on realignment of soft tissues and remodeling of distal ulnar physis. It has been described here for treatment of Type III and IV radial club hands and for patients with age equal to or less than 2 years at the time of primary surgical intervention. Advantage of this technique is that it involves minimal soft tissue dissection and is easily reproducible after a short learning curve.
Conclusion
Distraction techniques using monolateral and Ilizarov external fixators have an important role in the treatment of Congenital Radial club hand. They help lengthen the short radius and the shortened ulna along with deformity correction of the ulna either at the proximal or distal level. They ease the operations of centralization of the wrist by reducing the need for extensive soft tissue distraction. Recurrent deformities are easily corrected by distraction techniques. It aids displacement of the carpus to the ulnar border of distal ulna in Ulnarization. This procedure improves appearance of the hand by correcting the deformity, prevents its recurrence but preserves the mobility of the wrist.
References
1. McCarthy JJ, Kozin SH, Tuohy C, Cheung E, Davidson RS, Noonan K. External fixation and centralization versus external fixation and ulnar osteotomy: the treatment of radial dysplasia using the resolved total angle of deformity. J Pediatr Orthop 2009;29(7):797–803.
2. Saini N, Patni P, Gupta SP, Chaudhury L, Sharma V. Management of radial clubhand with gradual distraction followed by centralization. Indian J Orthop. 2009;43:292–300.
3. Ekblom AG, Laurell T, Arner M. Epidemiology of congenital upper limb anomalies in 562 children born in 1997 to 2007: a total population study from stockholm,sweden.J Hand Surg Am. 2010 Nov;35(11):1742-54.
4. Pardini AG Jr. Radial dysplasia. Clin Orthop Relat Res. 1968 Mar-Apr;57:153-77.
5. HEIKEL HV. Aplasia and hypoplasa of the radius: studies on 64 cases and on epiphyseal transplantation in rabbits with the imitated defect. Acta Orthop Scand Suppl. 1959;39:1-155.
6. Sayre RH. A contribution to the study of Club Hand. Trans Amer Ortho Assn. 1893;6:208–16.
7. M. Farzan. Congenital Radial Club Hand : Results of centralization in 10 cases Acta Medica Iranica,2005 Vol. 43, No. 1
8. Kawabata H, Yasui N, Ariga K, Shirata T. Bone lengthening with the Ilizarov apparatus for congenital club hands. Tech Hand Up Extrem Surg. 1998 Mar;2(1):72-7.
9. Kanojia RK, Sharma N, Kapoor SK. Preliminary soft tissue distraction using external fixator in radial club hand. J Hand Surg Eur Vol. 2008 Oct;33(5):622-7.
10. Albee FH. Formation of radius congenitally absent: condition seven years after implantation of bone graft. Ann Surg. 1928 Jan; 87(1): 105-10.
11. Medrykowski F, Barbary S, Gibert N, Lascombes P, Dautel G. Vascularized proximal fibular epiphyseal transfer: two cases. Orthop Traumatol Surg Res. 2012 Oct;98(6):728-32.
12. Ceulemans L, Degreef I, Debeer P, De Smet L. Outcome of index finger pollicisation. J Hand Microsurg. 2010 Jun;2(1):13-7.
13. Fujiwara M, Nakamura Y, Nishimatsu H, Fukamizu H. Strategic two-stage approach to radial club hand. J Hand Microsurg. 2010;2:33–7.
14. Sestero AM, Van Heest A, Agel J. Ulnar growth patterns in radial longitudinal deficiency. J Hand Surg Am 2006;31(6):960–967.
15. Damore E, Kozin SH, Thoder JJ, Porter S. The recurrence of deformity after surgical centralization for radial clubhand. J Hand Surg [Am]. 2000 Jul; 25(4):745-751.
16. Shariatzadeh H, Jafari D, Taheri H, Mazhar FN. Recurrence rate after radial club hand surgery in long term follow up. J Res Med Sci. 2009; 14(3):179-86.
| How to Cite this Article: Patwardhan S, Aneja K, Shyam AK. Percutaneous centralization for Radial Club Hand – a technical note International Journal of Paediatric Orthopaedics Sep-Dec 2016;2(3):19-23. |