The Use of Distraction Techniques in Treating Radial Clubhand
Volume 2 | Issue 3 | Sep-Dec 2016 | Page 12-15| Milind Chaudhary
Authors : Milind Chaudhary [1]
[1] Director, Centre for Ilizarov Techniques, Chaudhary Hospital, Akola, Maharashtra, India
Address of Correspondence
Dr Milind Chaudhary
Director, Centre for Ilizarov Techniques, Chaudhary Hospital, Akola, Maharashtra, India
Email: milind.chaudhary@gmail.com
Abstract
Radial club hand is a complex anomaly and requires customised approach. Distraction techniques are useful as alternative and adjunctive procedures +in various stages of management of radial club hand. The main use of distraction is to lengthen the ulna and correct its deformity and distraction prior to centralisation of hand reduce tissue dissection. Distraction can also be used as a precursor to microvascular joint transfer, to correct residual deformities in radial clubhand and as an adjunct to the operation of ulnarization The present article details the use of distraction techniques in radial club hand and provides insight into its principles based on authors experience.
Keywords: Distraction, radial club hand.
Introduction
Radial club hand or radial hemimelia is a difficult congenital anomaly to treat. There is a severe manus valgus deformity at the wrist due to a partial or complete absence of the radius. Movements of the elbow and interphalangeal joints of fingers are restricted. There is a high incidence of aplasia and hypoplasia of the thumb [1,2].
Treatment aims to correct deformity at the wrist to improve the appearance and hopefully the function as well. Untreated patients adapt well to the deformities and have reasonable function. The shortened forearm and deformed wrist are unsightly. Distraction techniques help lengthen and correct deformities of the bones. Distraction lengthens the shortened and deficient soft tissues as a precursor to centralization of the wrist. External fixation and distraction help assist Ulnarization of the wrist.
For lengthening & deformity correction of the bones
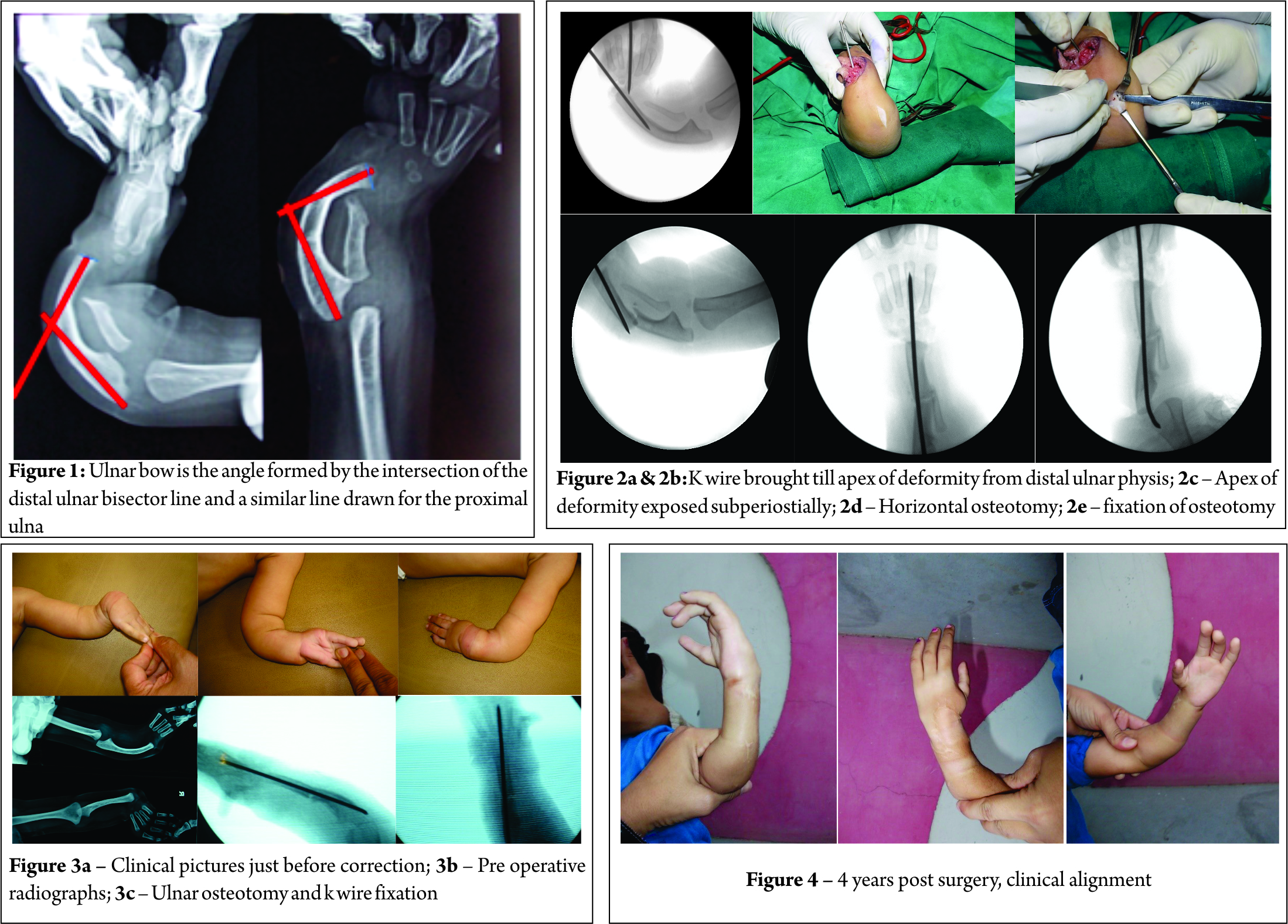
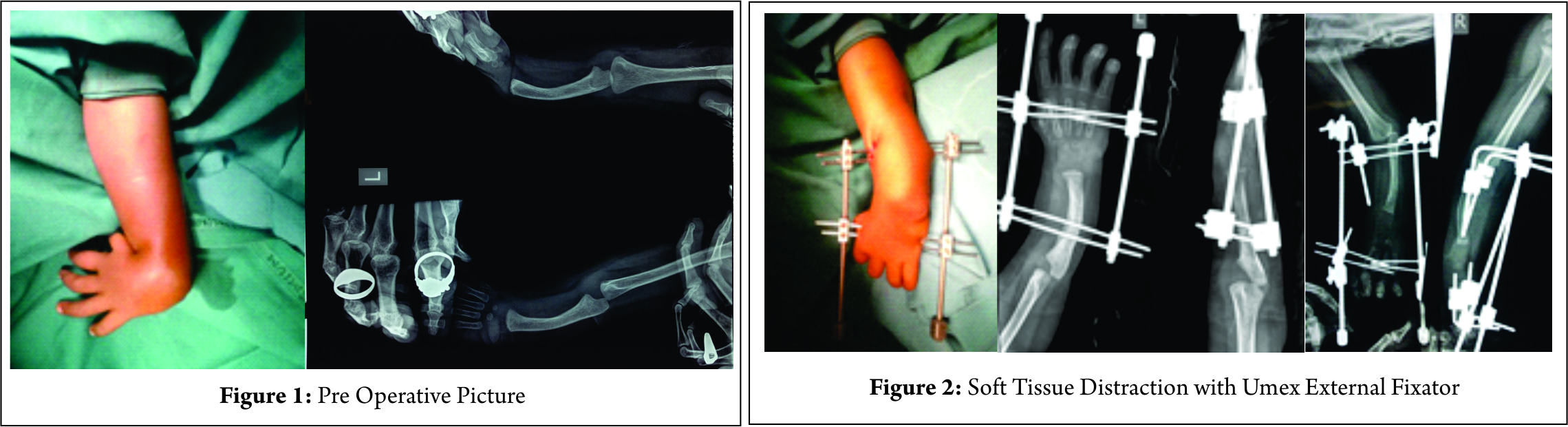
The condition occasionally presents itself as a shortening of the Radius. Distraction lengthening of the distal radius equalizes length to that of the ulna to match it at the distal radial ulnar joint [3,4]. Though uncommon, it is the simplest of all treatment modalities(Fig1).
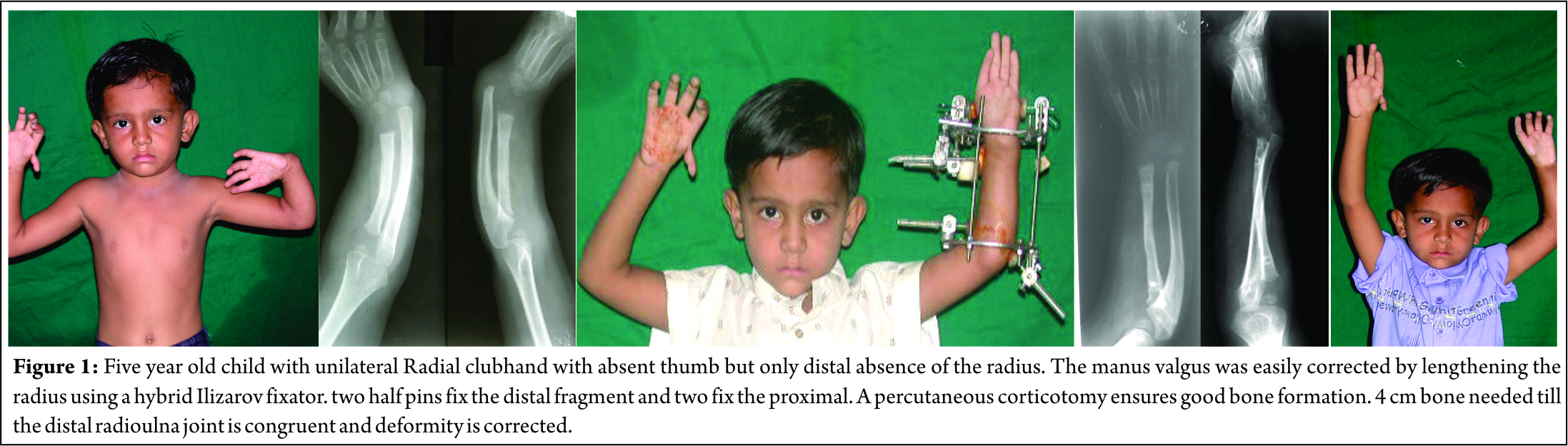
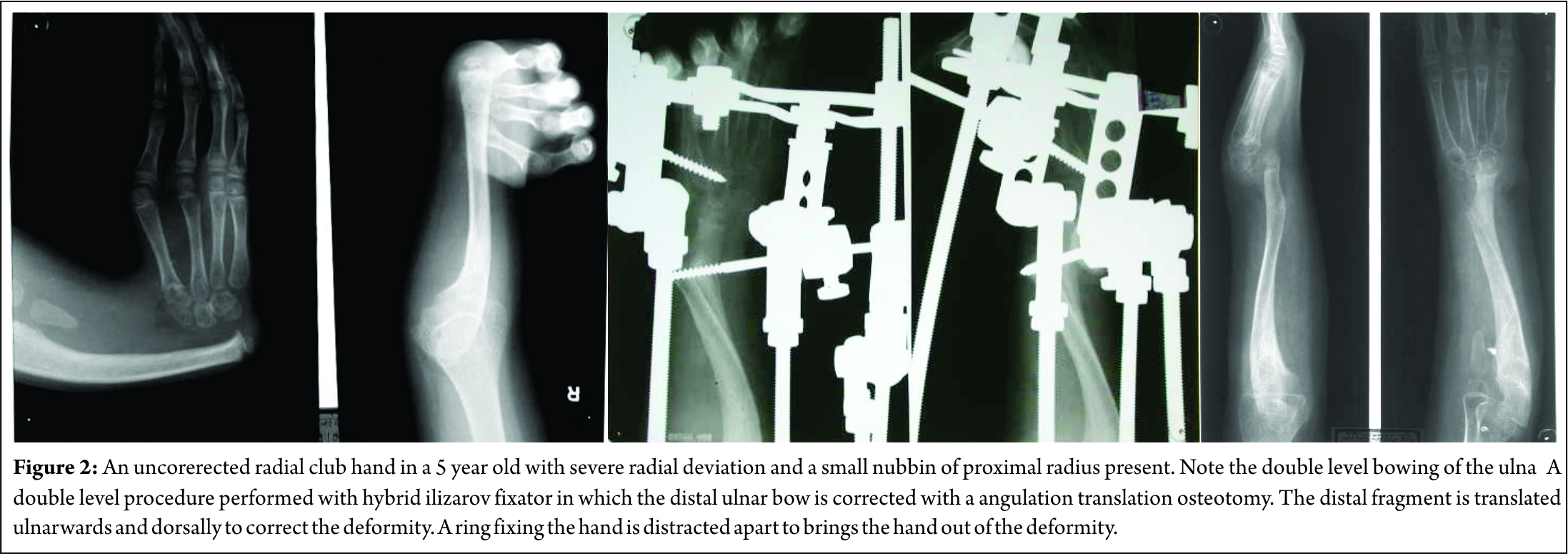
A monolateral fixator is easy to use with two half pins in the proximal and distal fragment each. An angulation translation osteotomy corrects the bowing deformity of the proximal ulna. A large deformity can be corrected percutaneously. In this situation, it is better to perform the surgery using the Ilizarov external fixator. A 5/8 th ring fixed proximally at the elbow is kept open anteriorly to allow flexion of the elbow joint. The distal ulnar ring can be a full one.
The hand is fixed with a ring with wires and half pins. Distraction in the concavity corrects the radial deviation deformity. The hand ring also prevents deformities that may arise with distraction.
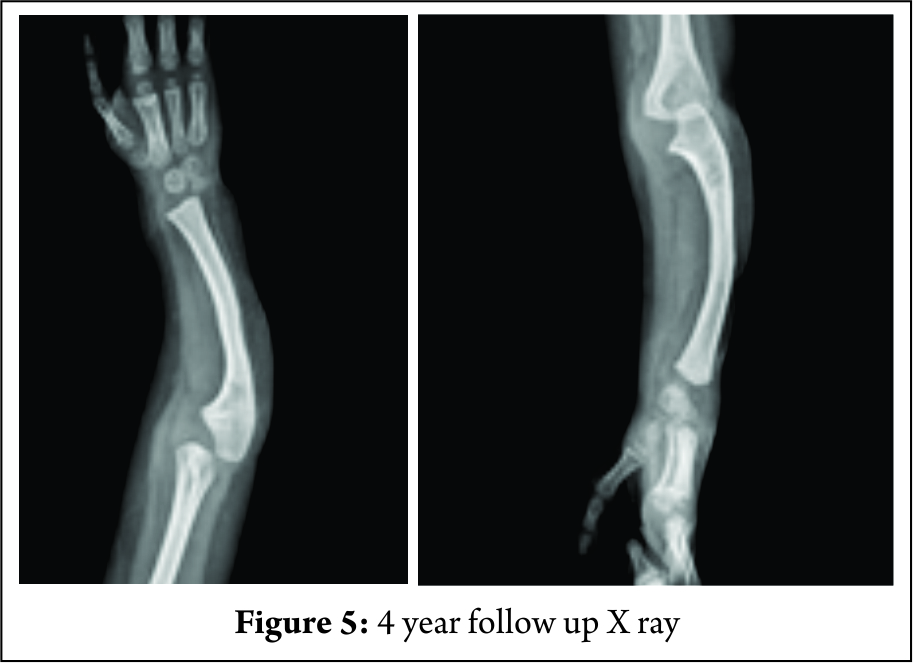
Deformity at the carpus can be corrected with an angulation-translation osteotomy of the distal ulna without resorting to open surgery. Ulnar bow is corrected by angulating the distal ulnar fragment with medial translation. This helps buttress the wrist and improve the appearance of the hand (Fig. 2).
Lengthening of the radius equalizes radio –ulnar length in acquired clubhand due to growth arrest. The aim is to correct the length deficit as well as angular deformity of the lower end of radius and to try and match it to the distal ulna [5,6] . The physeal arrest must also be addressed on its merits and a physeal bar resection must be performed.
The use of distraction techniques as a precursor to Centralization
Deformity correction by centralization is popular and the aim is to get the ulna to be collinear with the lunate, capitate and third metacarpal. Extensive soft tissue release with resection of the capsule is needed to get the carpus in line with the ulna. The deficiency of the soft tissues as well as skin on the radial side makes this a difficult task. Many have also described the role of pre-centralization distraction. It is an attractive concept as it may help reduce the extensive soft tissue dissection needed to get the carpus on top of the ulna. The soft tissue deficit causes radial deviation and ulnar subluxation of the wrist. Gradual distraction of the soft tissues doesn’t merely stretch them but lengthens them according to the law of tension stress [7]. A monolateral or circular external fixator is applied to the hand and ulna. Soft tissue elongation allows the hand to be distracted out of radial deviation & volar subluxation to enable the third metacarpal to become collinear with the ulna [ 8,9,10,11,12]. The external fixator retains the lengthened position till soft tissues mature & prevents reshortening. This may reduce the extent of soft tissue dissection needed to achieve correction.
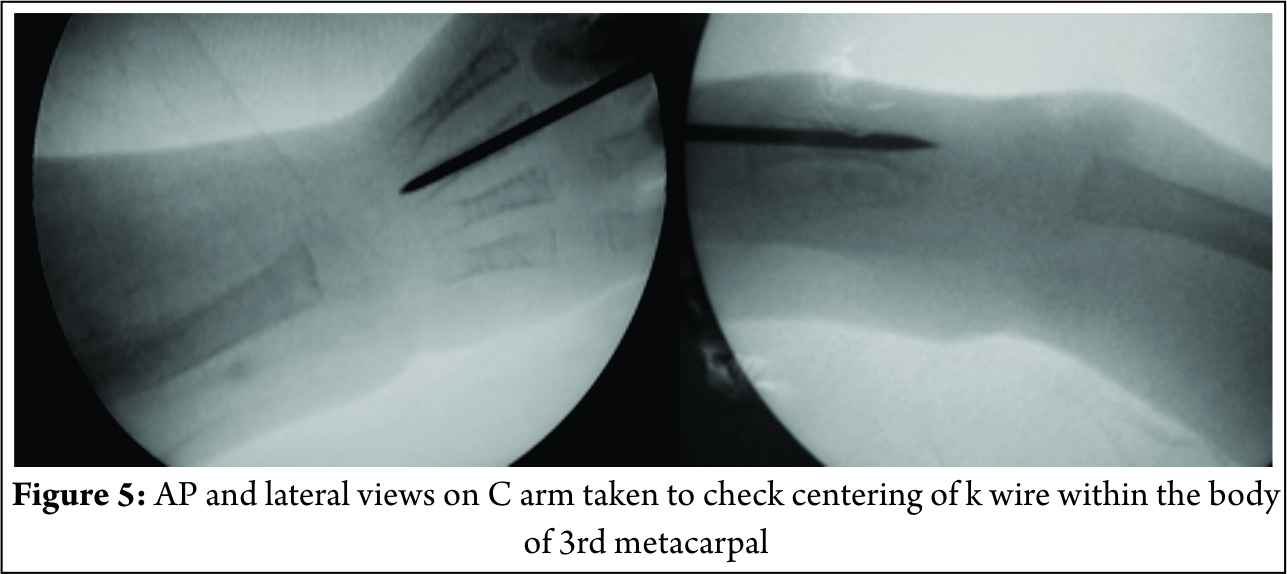
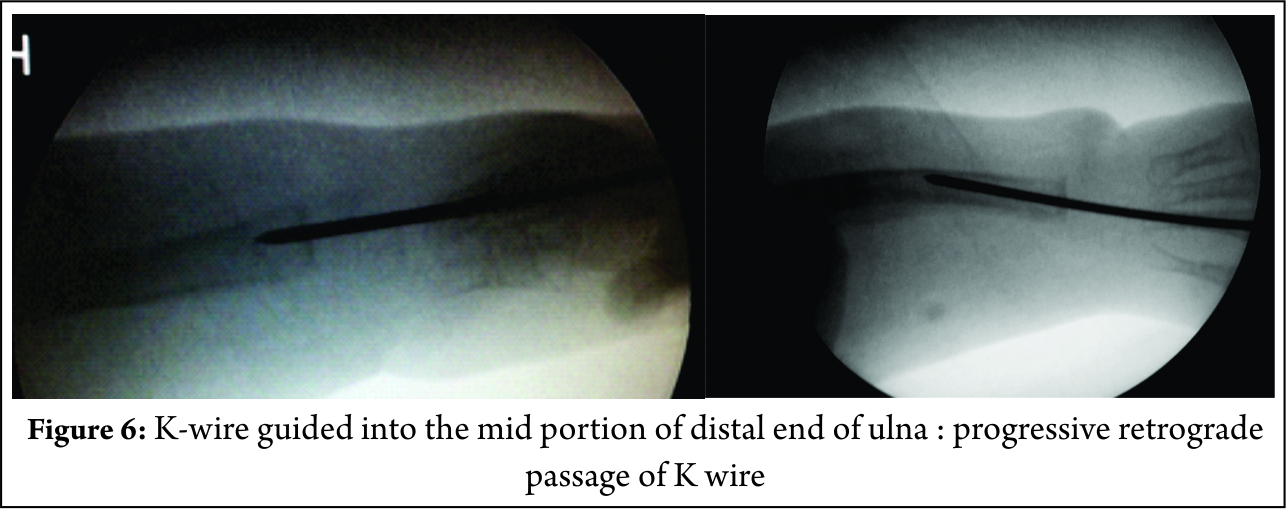
A K wire travels from the third metacarpal going down into the capitate, lunate and ulna. Some prefer to remove the K wire at 12 weeks and retain the correction by either tendon transfers or a brace. Some prefer to leave the K wire in situ. The K wire may be passed without making any preparatory changes in distal ulna. External fixation corrects the deformity maintains the position thereafter. The distal ulna flattens out to match the surfaces of the carpus. Preserved movement and improved appearance gives a good cosmetic and functional result.
The external fixator maintains position and stabilizes the wrist. Some surgeons create a notch in the proximal carpus and insert the distal ulna in it. The notch behaves like a multiplane joint to allow movement and prevents recurrence of deformity.
Distraction techniques as a precursor to Microvascular joint transfer
There is a complete deficit of the radial side of the wrist. Any positioning of the carpus on the distal ulna is therefore unstable. Distracting the carpus out of radial deviation and volar subluxation creates space on the radial side of the wrist. Microvascular technique is used to fill this space with the second metatarsal and metatarsophalangeal joint transfer. The bone is fixed to the ulna in a Y shaped manner [13,14]. The advantage of this method is that a proper joint is created and buttress support to the radial aspect of the wrist is permanent. However, long term studies are lacking on how these transfers perform. The microvascular technique itself is rather complex and such skills may not be available at all centres which makes their application rather limited.
Distraction techniques to correct residual deformities in Radial Clubhand
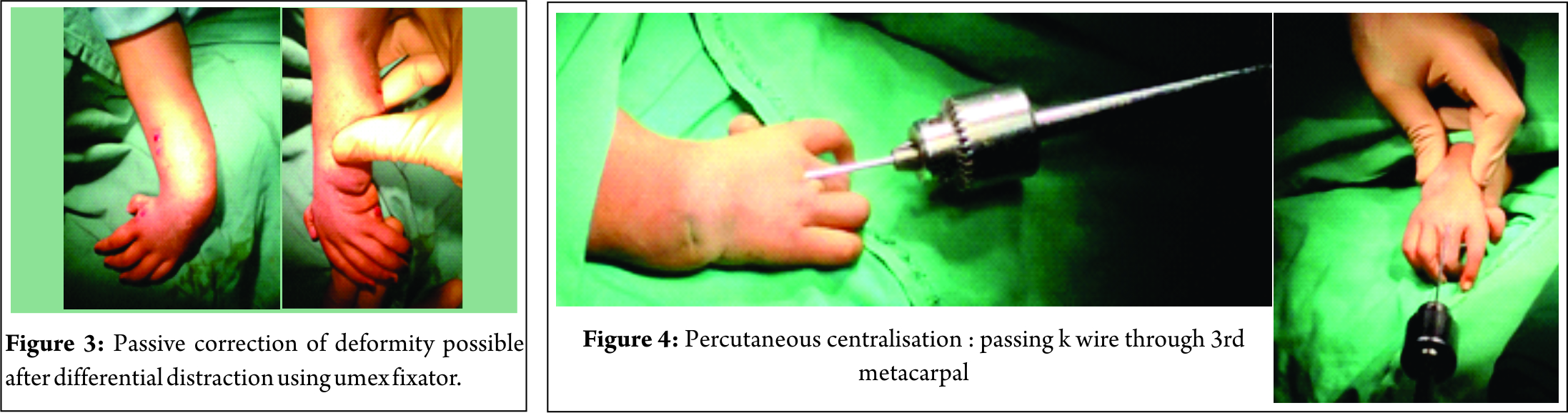
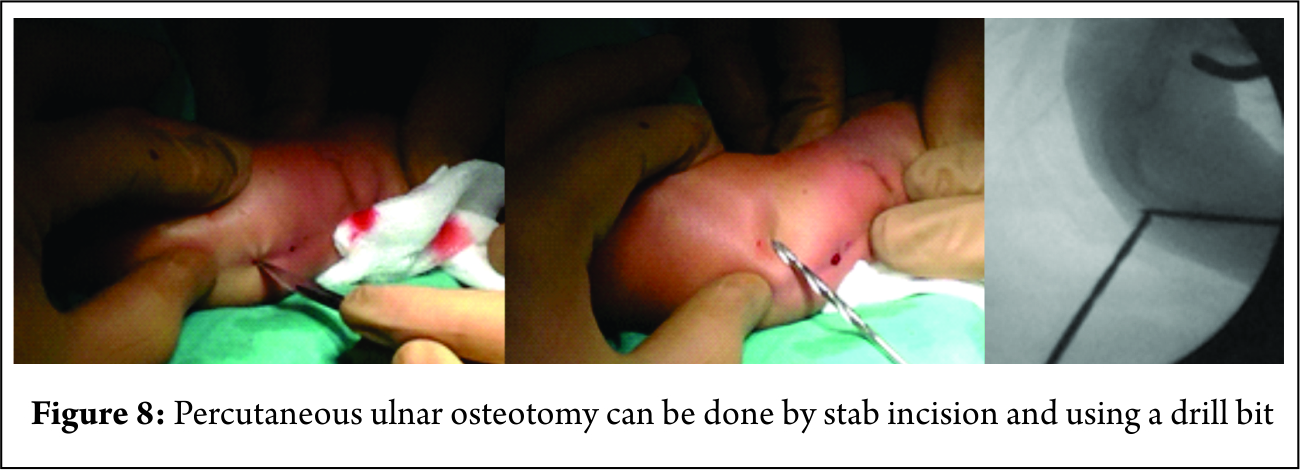
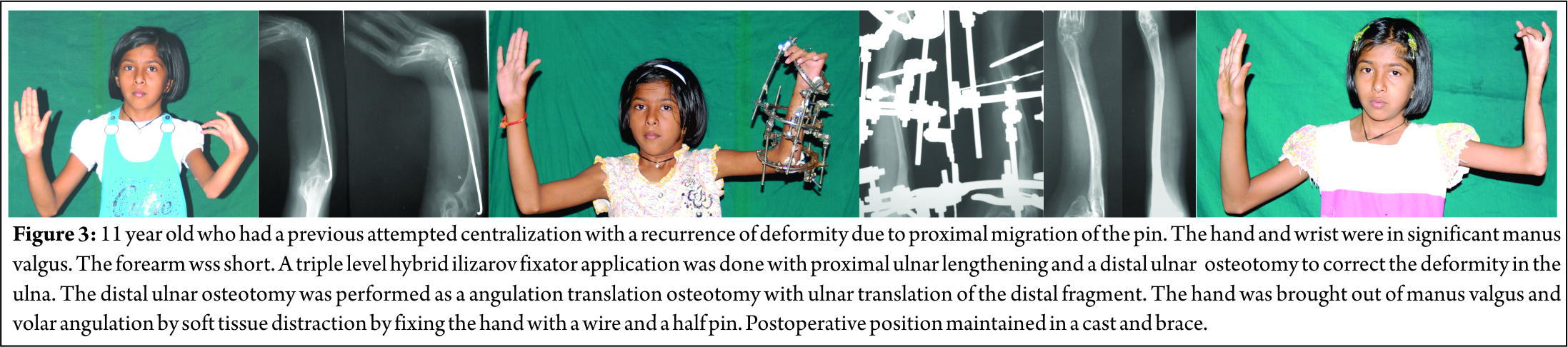
A common complication of centralization is recurrence of the deformity. Since K wires are removed after a few weeks (or may migrate proximally), recurrence of the deformity is likely due to re-shortening of the fibrotic and inelastic soft tissues. The extensive dissection of the distal ulna may damage its blood supply and result in distal ulnar growth arrest with deformities and shortening. In these situations, a circular external fixator [15,16,17] can easily correct the residual deformity by soft tissue distraction of the hand and wrist. The hand is brought out of the radial deviation and volar subluxation and repositioned on top of the distal ulna. Passing a K wire, or creating a trough for the ulna or by a wrist arthrodesis creates stability. Prolonged bracing may also help. Percutaneous osteotomy helps correct deformities at any level in the ulna. Proximal ulnar lengthening can be added as well. (Fig. 3)
Corticotomy lengthening and gradual correction of the angular deformity are possible in the proximal ulna. Compression between the distal ulna and carpus helps fuse the wrist.
Distraction as an adjunct to the operation of Ulnarization
Wrist and finger movement are more important than maintenance of hand forearm angle for long term hand function [18]. However, fingers are usually stiff to start with and cannot be influenced by surgery. Centralization or radialization reduce movement at the wrist even without fusion. Recurrence of the radial deviation and volar subluxation deformity of the wrist is common.
Creating a notch in the wrist with residual deformity may eventually need an arthrodesis. Combined with the restricted movements in the elbow and PIP and DIP joints of the fingers stiffness of the wrist can contribute to functional disability.
Paley described Ulnarization to correct the deformity, retain movement at the wrist and prevent its recurrence [19]. This is an advanced technique of reconstruction of the deformities of radial clubhand. It prevents the problems associated with the previous methods of treatment, namely: recurrence of the deformity, stiffness of the wrist and distal ulnar growth arrest.
Ulnarization shifts the wrist and hand from radial to the ulnar side of the distal ulna. The ulnar border of the distal ulna mechanically prevents radial deviation of the wrist. (Fig. 4).
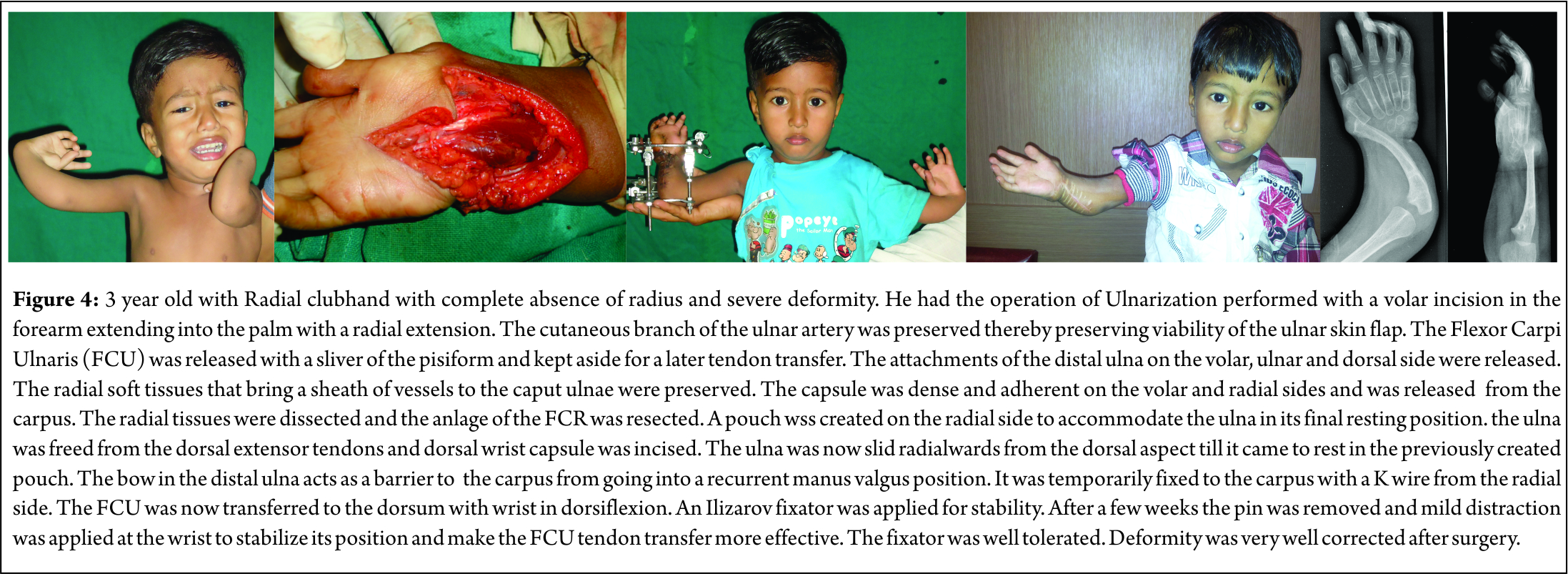
The second part of the operation transfers the flexor carpi ulnaris tendon from the pisiform to the dorsal side of the wrist. The operation can be performed as early as 15-18 months of age. Magnification with a surgical loupe helps preserve small vessels in surgery in very young children. Pollicization of the index finger can be performed at a later date.
The incision begins at ulnar border of lower humerus, extends across the forearm, goes towards radial aspect wrist and then back along the wrist crease in a Z to open in the palm. The radial extension helps to create a pocket on the radial side of the distal forearm and wrist joint in which the distal ulna can be translocated. The blood supply to the distal ulnar epiphysis comes from the radial side and should be preserved while freeing the distal ulna from the wrist capsule. The tendons dorsal to ulna are released by sharp dissection from the distal ulna. Complete release of capsule from the radial, volar and dorsal sides helps mobilize the distal ulna.
Gentle dissection creates a pocket on the radial side of the distal forearm allowing the distal ulna to slide from the dorsum of the wrist towards its radial aspect. Care is taken to prevent subluxation of wrist and hand on the volar or dorsal side of distal ulna. It is fixed to the hand and wrist with a K-wire for a few weeks. Ilizarov fixator fine tunes position of the hand and wrist on the distal ulna. It may also be used for an osteotomy of the proximal ulna if grossly deformed. The distal ring is distracted to improve the tension in the soft tissues and transferred tendons.
Prominence of the distal ulna on the radial side of the wrist looks like a prominent radial styloid. The appearance of the entire forearm and hand is dramatically improved. The FCU is transferred to the dorsal ulnar side of the wrist to the base of the fifth metacarpal. The wrist can dorsiflex due to transferred action of flexor carpi ulnaris. Muscles on the radial side of the wrist are usually absent and unavailable for tendon transfers.
The author has performed five procedures in four patients over the last seven years. Age has ranged from 2 to 18 years of age. Follow-up has now ranged from a period of three years to eight years. A short period of bracing or casting was needed in two of our cases. The improved appearance of the hand was satisfactory for all of our patients. There was a mild recurrence of the volar flexion deformity at the wrist in 2 of five patients. There was very little recurrence of radial deviation deformity. Three had aplasia of the thumb for which they have not yet come for pollicisation. Poor hand function has been chiefly due to lack of the thumb and stiffness of the fingers.
Conclusion
Distraction techniques using monolateral and Ilizarov external fixators have an important role in the treatment of Congenital Radial club hand. They help lengthen the short radius and the shortened ulna along with deformity correction of the ulna either at the proximal or distal level. They ease the operations of centralization of the wrist by reducing the need for extensive soft tissue distraction. Recurrent deformities are easily corrected by distraction techniques. It aids displacement of the carpus to the ulnar border of distal ulna in Ulnarization. This procedure improves appearance of the hand by correcting the deformity, prevents its recurrence but preserves the mobility of the wrist.
References
1. Lamb DW. Radial club hand. A continuing study of sixty-eight patients with one hundred and seventeen club hands. J Bone Joint Surg Am. 1977 Jan;59(1):1-13.
2. Bora FW Jr, Osterman AL, Kaneda RR, Esterhai J. Radial club-hand deformity. Long-term follow-up. J Bone Joint Surg Am. 1981 Jun;63(5):741-5.
3. Tetsworth K, Krome J, Paley D. Lengthening and deformity correction of the upper extremity by the Ilizarov technique. Orthop Clin North Am. 1991;22: 689-713.
4. Takagi T, Seki A, Mochida J, Takayama S. Bone lengthening of the radius with temporary external fixation of the wrist for mild radial club hand. J Plast Reconstr Aesthet Surg. 2014 Dec;67(12):1688-93.
5. Zhang X, Duan L, Li Z, Chen X. Callus distraction for the treatment of acquired radial club-hand deformity after osteomyelitis. J Bone Joint Surg Br. 2007 Nov;89(11):1515-8
6. Hosny GA, Kandel WA. Treatment of posttraumatic radial club hand with distraction lengthening. Ann Plast Surg. 2013 Nov;71(5):489-92.
7. Ilizarov G.A. Clinical effect of the tension stress effect for limb lengthening. Clin. Orthop. Rel. Res.1990 Jan (250) 8: 26.
8. Sabharwal S, Finuoli AL, Ghobadi F. Pre-centralization soft tissue distraction for Bayne type IV congenital radial de¬ficiency in children. J Pediatr Orthop 2005;25(3):377-81.
9. Kanojia RK, Sharma N, Kapoor SK. Preliminary soft tissue distraction using external fixator in radial club hand. J Hand Surg Eur Vol. 2008 Oct;33(5):622-7.
10. Thirkannad SM, Burgess RC. A technique for using the Ilizarov fixator for primary centralization in radial clubhand. Tech Hand Up Extrem Surg. 2008 Jun;12(2):71-8.
11. Saini N, Patni P, Gupta S, Chaudhary L, Sharma V. Management of radial clubhand with gradual distraction followed by centralization. Indian J Orthop. 2009 Jul;43(3):292-300.
12. Bhat SB, Kamath AF, Sehgal K, Horn BD, Hosalkar HS. Multi-axial correction system in the treatment of radial club hand. J Child Orthop. 2009 Dec;3(6):493-8.
13. Vilkki SK. Distraction and microvascular epiphysis transfer for radial club hand. J Hand Surg Br. 1998 Aug;23(4):445-52.
14. de Jong JP, Moran SL, Vilkki SK. Changing paradigms in the treatment of radial club hand: microvascular joint transfer for correction of radial deviation and preservation of long-term growth. Clin Orthop Surg. 2012 Mar;4(1):36-44.
15. Kawabata H, Shibata T, Masatomi T, Yasui N. Residual deformity in congenital radial club hands after previous centralisation of the wrist. Ulnar lengthening and correction by the Ilizarov method. J Bone Joint Surg Br. 1998 Sep;80(5):762-5.
16. Damore E, Kozin SH, Thoder JJ, Porter S. The recurrence of deformity after surgical centralization for radial clubhand. J Hand Surg Am. 2000 Jul;25(4):745-51.
17. Shariatzadeh H, Jafari D, Taheri H, Mazhar FN. Recurrence rate after radial club hand surgery in long term follow up. J Res Med Sci. 2009 May;14(3):179-86.
18. Hand function in children with radial longitudinal deficiency Anna Gerber Ekblom, Lars B Dahlin, Hans-Eric Rosberg, Monica Wiig, Michael Werner, Marianne Arner BMC Musculoskeletal Disorders 2013, 14:116.
19. Paley D, Robbins CA. Ulnarization for treatment of radial club hand. Limb Lengthening & Reconstruction Surgery Case Atlas. Switzerland, Springer International 2015 Jan:1-11.
| How to Cite this Article: Chaudhary M. The use of distraction techniques in treating radial clubhand. International Journal of Paediatric Orthopaedics Sep-Dec 2016;2(3):12-15. |