Ulna Osteotomy Role – Methods, Timing, Combo Procedures, Recurrences and Re- Osteotomy
Volume 2 | Issue 3 | Sep-Dec 2016 | Page 16-18| Premal Naik, Hitesh Chauhan
Authors : Premal Naik [1], Hitesh Chauhan [1]
[1] Rainbow Rainbow Super Speciality and Children Orthopaedic Hospital, Ahmedabad.
Address of Correspondence
Dr Premal Naik
Rainbow Rainbow Super Speciality and Children Orthopaedic Hospital, Ahmedabad.
Email: premalnaik@gmail.com
Abstract
Ulna bowing is common occurrence in radial club hand and depends on the severity of the deformity. Centralisation takes care of the wrist stability and deformity however ulna deformity if ignored may continue to progress and cause significant forearm deformity. Current recommendation it to perform Ulna osteotomy at the time of index procedure of centralisation, if the ulna deformity is more than 30 degrees. Current article describes the technique and methods of ulna osteotomy.
Keywords: Ulna osteotomy, radial club hand.
Introduction
Congenital radius deficiency, or radial hemimelia, is characterized by a hypoplasia or complete absence of the radius. In radial hemimelia, ulnar bowing plays a significant role in overall deformity. Severity of ulnar bowing is mostly proportional to severity of radial hypoplasia.
Centralization for correction of radial hemimelia was proposed in 1894 [8] and has been modified later on by many surgeons [1, 2, 6, 7, 10]. It has shown significant improvement in overall wrist function and strength but correction of forearm deformity i.e. correction of ulnar bow has not been given due importance.
Progressive ulnar bowing is an important late complication after centralization surgery, when forearm deformity is severe and is not corrected [1, 5, 9]. There remains a dilemma whether to correct ulna bowing during the index procedure or to perform it at a second stage.
Ulnar bowing – Current scenario
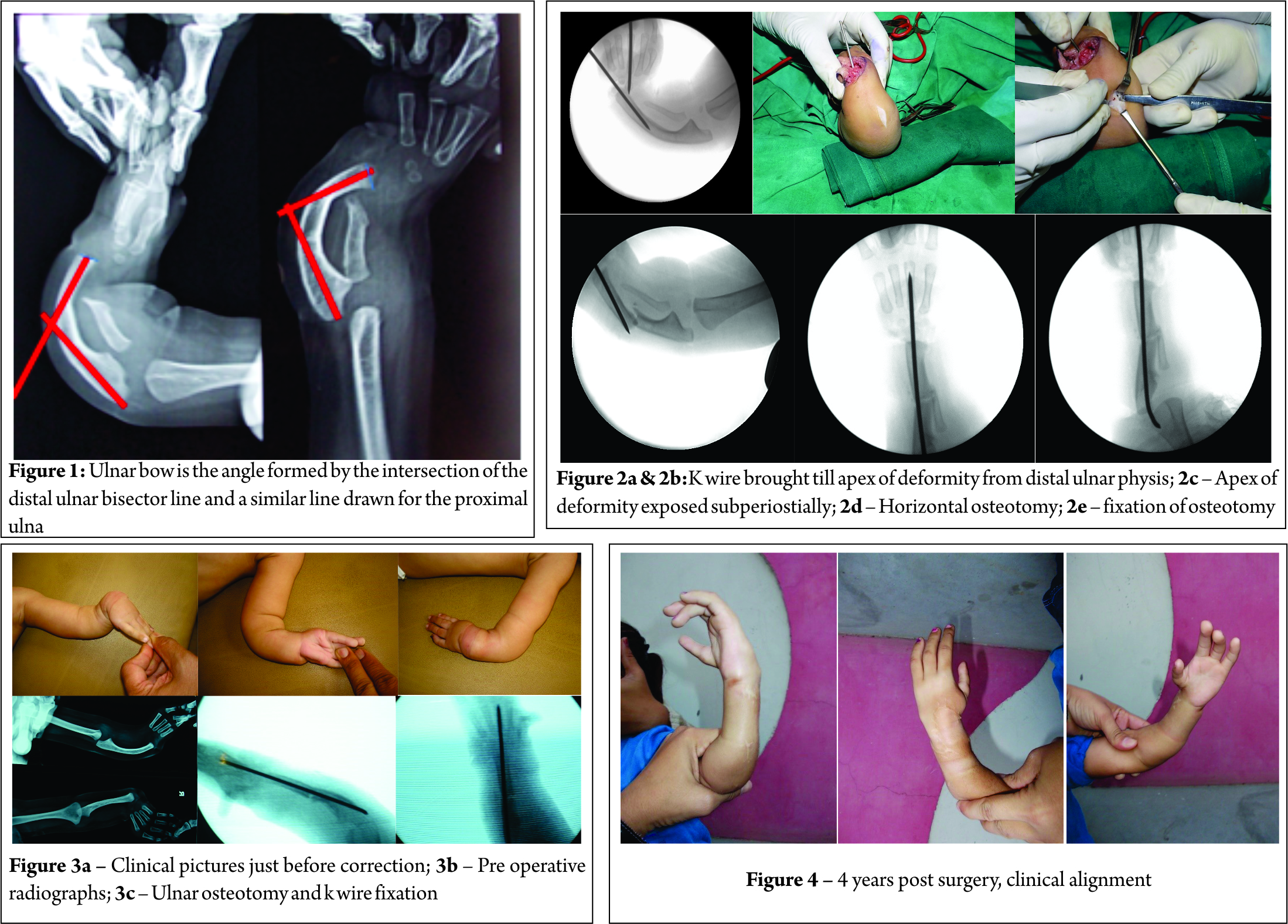
Ulnar bow is the angle formed by the intersection of the distal ulnar bisector line and a similar line drawn for the proximal ulna (Fig.1) [3]. Severity of forearm deformity depends on the severity of radial hypoplasia. Radial hemimelia with complete absence of radius (Bayne and Klug type III & IV) present with severe forearm deformity as compared to mild hypoplasia (Bayne and Klug type II).
According to Bayne and Klug and few other reports, ulnar bow was considered to be significant if angular deformity is more than 30°. They did not recommend corrective osteotomy of the ulna if the angular deformity was less than 30° [1] .
According to Geck MJ et.al ulnar osteotomy was performed for ulnar bow greater than 30° and for milder deformity of less than 30° it was done only if needed, to pass the transfixing pin[3].
Timing and method of ulna osteotomy is not defined clearly in literature and depends on surgeon’s preference. It is either performed during index procedure or can be done at a second stage[3, 9]. Few surgeons prefer to correct ulnar angulation at the time of lengthening[4].
In Geck MJ et.al series, 13 ulnar osteotomies were performed along with index procedure and 4 osteotomies were done as secondary procedure. The ulnar osteotomy was performed at the apex of deformity when deformity is more than 30° and in less severe deformity, it was performed wherever k wire could not be passed thorough ulnar shaft. Osteotomy was transfixed with same k wire, which is fixing the wrist. Wire was removed at 8 – 12 weeks. They noted no statistically significant difference of results between osteotomy done along with index procedure or as secondary procedure at the final follow-up. They could achieve statistically significant correction in ulnar bow from preoperative measurement to final follow-up measurement and found that Ulnar osteotomy did not have a deleterious effect on the correction of the wrist deformity [3].
H. Kawabata and colleagues recommended correction of congenital radial club hand by staged procedures. The first is centralization followed by lengthening of the ulna and correction of the angular deformity using the Ilizarov method. In their series mean angular deformity was 42°. Full correction of angular deformity was done in six out of seven patients but at final follow up mean correction was 57 % of initial correction [4].
Deformity recurrence and revision is an important issue in surgical correction of congenital radius deficiency. Revision surgery is mostly attributed to recurrent increased hand forearm angle or increased radial translation at wrist as compared to recurrence of ulnar bow[4, 9].
Due to poor growth potential of ulnar physis, recurrence of forearm deformity after correction is mostly not significant[4]. Geck MJ showed that there was no statistically significant difference between the postoperative and final follow up ulnar bow in patients with and without ulnar osteotomy[8].
According to H. Kawabata, recurrence of ulnar bowing was due to muscle imbalance which was exaggerated by the lengthening. The recurrence was least in a wrist with well-balanced muscle forces. So they proposed first centralization procedure is of great importance for further Illizarov correction[4] .
Authors preferred treatment
We routinely take ‘All In One’ approach for correction of radial club hand. This includes single stage, centralization with tendon transfer and Ulna Osteotomy. Addition of ulnar osteotomy adds very little time and obviates the need for second surgery. In our center we have operated 45 extremities in 40 patients till May 2016. We presented our experience of 24 extremities in 20 patients earlier (POSICON 2013). We could achieve statistically significant improvement in wrist forearm angle and ulnar angulation in all patients. Ulnar angulation was corrected from an average of 380 preoperatively to 130 postoperatively (p value – < 0.0001) and wrist forearm angle was corrected from an average of 410 preoperatively to 130 postoperatively (p value – < 0.0001). We did not have any significant problem related to ulnar osteotomy. We found ulnar osteotomy a useful adjunct in the treatment of radial hemimelia.
Surgical technique
We use either Ewan bilobed flap of lazy S incision. After exposing the wrist a provisional track is made with k wire from distal ulnar epiphysis till apex of deformity (Fig 2a, b). One K wire is then passed from 3rd MC head transfixing carpus over distal ulna and advanced in distal ulnar shaft till apex of deformity (in previously made tract).
Nail tip (at the apex of the deformity) is confirmed under image intensifier guidance. Apex of bow exposed subperiosteally (Fib 2 c) and horizontal osteotomy is done (Fig 2 d), k wire is then advanced in proximal fragment under vision and brought out through tip of olecranon (Fig 2 e). In severe deformities, minimal shortening is done to correct the deformity to avoid excessive stretch and injury to neurovascular bundle. After fixation of wrist and ulna osteotomy, tendon transfer is performed. AE cast is given for 6 weeks, followed by strict splinting. K wire is kept for at least 6 months post operatively. Fig. 2 describes the surgical technique
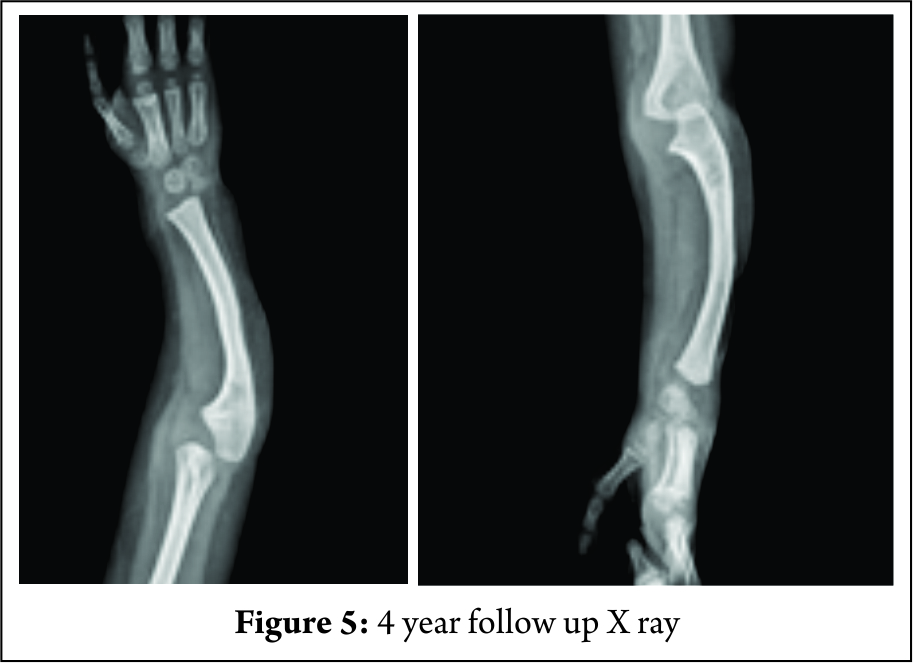
Illustrated Case: Two month old male child, presented with left radial hemimelia(Fig 3 a). On radiological evaluatoin, there was complete absence of radius with gross bowing of ulnawith pre operatively ulnar angulation of 400 (Fig 3 b) . He underwent ‘All In One correction’ at age of 10 months (Fig 3 c). Child under went pollicisation 1 year after primary surgery. After 4 year child is having good hand function and very good overall wrist and forearm allignment (Fig – 4). On follow up, ulnar angulation was 150 (Fig. – 5).
Conclusion
We have found ulnar osteotomy (along with centralisation and tendon transfer) a very useful and powerful tool in managing radial hemimelia. Ulnar osteotomy adds extra 20-300 correction in a significantly deformed upper limb.
Ulnar osteotomy is a simple procedure and does not add significant extra surgical time. We did not have any significant complications related ulnar osteotomy. We recommend ulnar ostetomy in all cases when angulaton is > 300 or when k wire can not be passed straight through the ulna.
References
1. Bayne LG, Klug MS. Long-term review of the surgical treatment of radial deficiencies. The Journal of hand surgery. 1987;12:169-179.
2. Buck-Gramcko D. Radialization as a new treatment for radial club hand. The Journal of hand surgery. 1985;10:964-968.
3. Geck MJ, Dorey F, Lawrence JF, Johnson MK. Congenital radius deficiency: radiographic outcome and survivorship analysis. The Journal of hand surgery. 1999;24:1132-1144.
4. Kawabata H, Shibata T, Masatomi T, Yasui N. Residual deformity in congenital radial club hands after previous centralisation of the wrist. Bone & Joint Journal. 1998;80:762-765.
5. Lourie GM, Lins RE. Radial longitudinal deficiency. A review and update. Hand clinics. 1998;14:85-99.
6. Manske PR, McCarroll HR, Swanson K. Centralization of the radial club hand: an ulnar surgical approach. The Journal of hand surgery. 1981;6:423-433.
7. Riordan D. Congenital Absence Of The Radius-a 15-year Follow-up. In: Journal Of Bone And Joint Surgery-american Volume. Journal Bone Joint Surgery Inc 20 Pickering St, Needham, Ma 02192: 1963:1783-1783.
8. Sayre RH. A contribution to the study of club-hand. Trans Am Orthop Assoc. 1894;1:208-216.
9. Shariatzadeh H, Jafari D, Taheri H, Mazhar FN. Recurrence rate after radial club hand surgery in long term follow up. J Res Med Sci. 2009;14:179-186.
10.. Watson HK, Beebe RD, Cruz NI. A centralization procedure for radial clubhand. The Journal of hand surgery. 1984;9:541-547.
| How to Cite this Article: Naik P, Chauhan H. Ulna Osteotomy Role – Methods, timing, combo procedures, recurrences and re- osteotomy. International Journal of Paediatric Orthopaedics Sep-Dec 2016;2(3):16-18. |