
Osteosynthesis in a 10 year old boy with Fracture neck of Femur, Infected Nonunion with Implants In-situ, Neck Resorption and Avascular Necrosis -A case report.
Vol 1 | Issue 1 | July-Sep 2015 | page:48-50 | EG Mohan Kumar, GM Yathish Kumar.
Authors : EG Mohan Kumar[1], GM Yathish Kumar[1].
[1] Department Of Orthopedic Surgery, KIMS Al Shifa Hospital, Perintalmanna, Kerala, India.
Address of Correspondence
Dr. EG Mohan Kumar
HOD Department Of Orthopedic Surgery, KIMS Al Shifa Hospital,
Perintalmanna, Kerala- 679322 India.
Email- orthomohan@rediffmail.com.
Abstract
Background: Non union fracture femoral neck is one of the common complication of intra capsular fracture neck of femur in children as well as in adults and it is the most challenging problem to treat if femoral head salvage is attempted. Other common complication is avascular necrosis (AVN) of the femoral head with most reported incidences being <15% (range 0% to 67%), which is similar to the complication rate with non-neglected femoral neck fractures. We are reporting a case of 10 year old boy who elsewhere underwent closed reduction and internal fixation with canulated cancellous screw for Delbert type III fracture neck of femur, which subsequently got infected with a draining sinus, non union and AVN of femoral head with complete absorption of the neck in 4 months time. We received the patient at that stage. He was managed by two stage surgery. Initially the implants were removed the screw tracks were curetted out and filled with antibiotic sponge. After the infection was eradicated osteosynthesis and neck reconstruction was done using fibular strut and cancellous grafts through modified Watson Jones approach and anterior capsulotomy . We avoided metal implants for fear of infection and so also a subtrochenteric osteotomy which require fixation. A hip spica cast was given for 6 weeks. The neck length was restored, vascularity restored and fracture united with an excellently functioning hip.
Keywords: Femur neck fracture, infection, osteosysnthesis.
Introduction
Fractures of the femoral neck in children are not common[1]. They represent fewer than 1% of all the paediatric fractures2. However, complications accompanying these fractures are frequent—specifically avascular necrosis, non union and early closure of the proximal physis of the femur—resulting in decrease of neck length and coxa vara. The incidence of non union varies from 7 to 10%, depending on the location of the fracture in the neck of femur[2,3,4]. Delbet was the first to describe the fractures of the femoral neck. He published the first classification in the French literature. Since then, Colonna[5] has quoted the Delbet classification, which is still accepted in all the literature regarding this subject, and Ratliff[6] has described the evaluation criteria of the results, based on the presence of pain, joint mobility and the child’s capacity to maintain a daily activity. Most of the articles in the literature support bone grafting and a valgus osteotomy with some sort of fixation[7]. Only few cases reported with non union neck of femur treated by fibular strut graft alone without fixation and osteotomy. We feel that our case was unique due to presence of infection which makes the situation complicated. Here, we report a case of paediatric femoral neck fracture which went in for all described complications like AVN, non union, infection and neck resorption which was managed successfully by staged surgery. In the first stage eradication of infection and in second stage osteosynthesis and neck length restoration was attempted.
Case Presentation
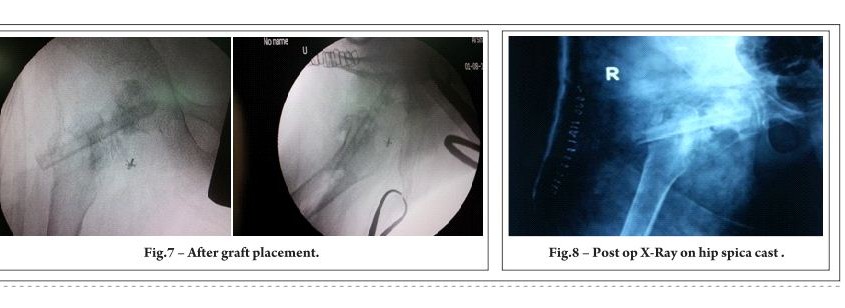
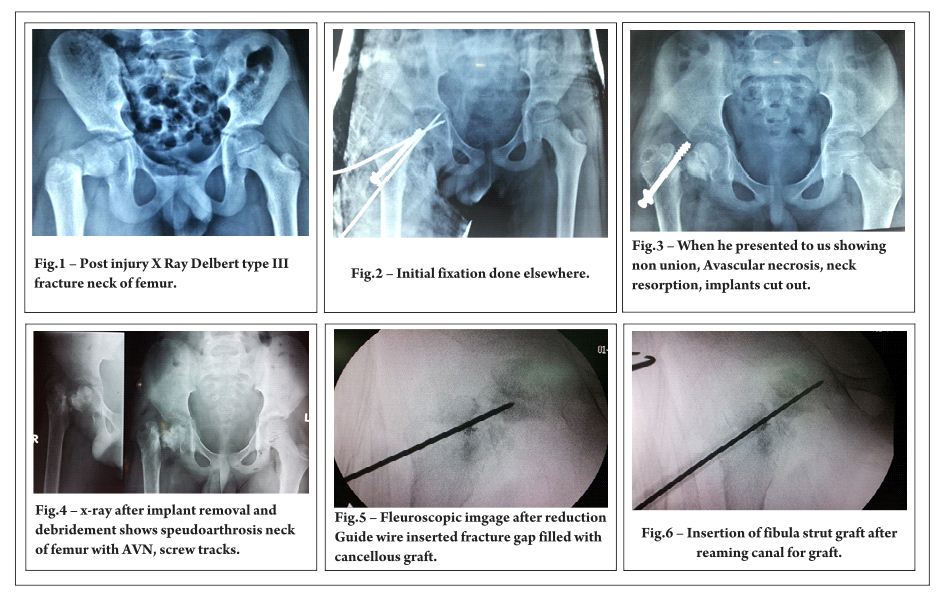
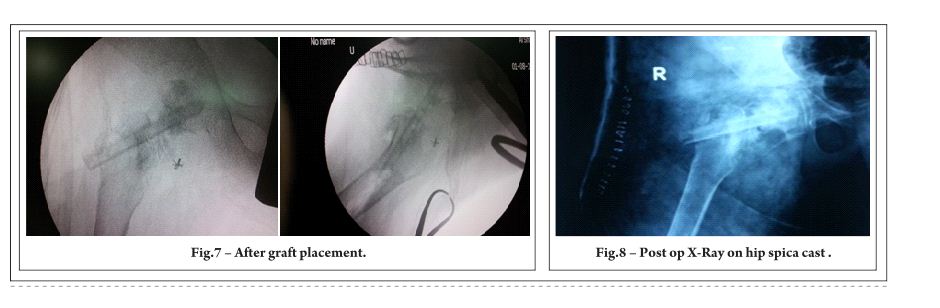
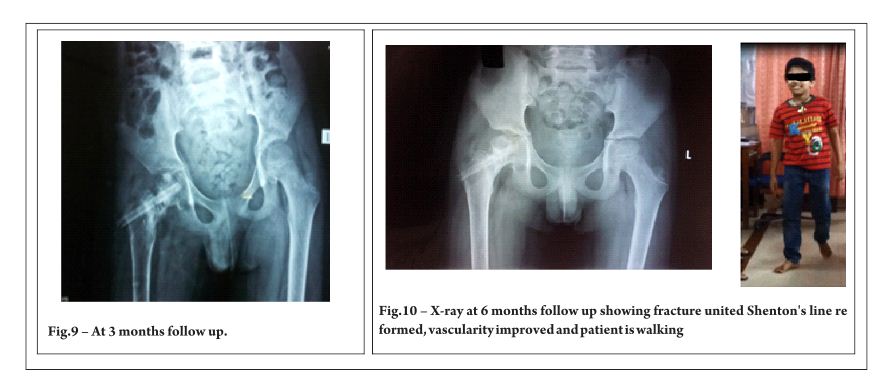
A 10 year old boy sustained fracture neck of right femur following fall from tree 4 months back(Fig.1) and was initially treated elsewhere by closed reduction and Canulated Cancellous Screw and K wire fixation(Fig.2), but osteosythesis was failed due to infection and poor fixation. He presented to us with non union, neck resorption, avascular necrosis of head of femur and infection with implants insitu(Fig.3). His WBC count(13000cells/cumm), ESR(40mmhg/hour) and CRP(110) were elevated. X-Ray showed loosening of implants with surrounding osteolysis and he was managed in two stages. Initially implants were removed, debridement was done, screw tracks were curetted out and antibiotic sponge was kept inside the tracks and was put on antibiotics(Fig.4). Once the infection got settled when CRP became normal after two months he was taken up for second stage surgery. He was treated by autologous fibular strut grafting and cancellous graft packing through Modified Watson Jones approach. Intra-operatively he was put on traction table, reduction and alignment was checked under C-ARM guidance(Fig.5), we could restore the length of neck with fibula graft under C-ARM guidance and cancellous gaft harvested from iliac crest was filled around fibula graft bridging fracture site through anterior capsulotomy(Fig.6,7). Patient was immobilized in hip spica cast for 6 weeks(Fig.8), POP was removed and X-ray taken .Gradually hip and knee were mobilized. He was reviewed every month with radiograph which showed good union of fracture and vascularity of the head of femur spontaneously improved(Fig.9,10). Made partial weight bearing with the support of walker at 3 months post op and gradually increased weight bearing. Fracture consolidated by 6 months. At present his fracture is completely united, vascularity of head of femur regained(Fig.10). He has got 1cm shortening of limb and patient is back to school walking without support without any pain. Since the proximal physis is fused he may develop an increase in the present limb length discrepancy which we plan to correct later.
Discussion
Fracture neck of femur in children is a rare injury and can lead to many complications. Nonunion and AVN are very common complication which is nearly equal in neglected and treated cases of fracture neck of femur[8].Infection further adds to challenge in treating these cases. We got chance to treat such a patient with failed osteosynthesis neck of femur with all known complication like infection, pseudoarthrosis, avascular necrosis and neck resorption. Investigation of nonunion of neck of femur should include TC,DC,ESR and CRP to rule out infection especially in failed osteosynthesis, MRI may be required if x-ray features are not conclusive of vascular status of head of femur. In the literature there are few articles about treating this challenging problem. All are supporting valgus osteotomy some sort of fixation, few are supporting fibular grafting and cancellous screw fixation[4,9], but all concerning situations without infection. We planned to tackle the infection first and go for osteosynthesis with bone grafting alone without osteotomy or use of any hardware for fixation, in view of the subsided infection. Fibular strut graft gave a very good structural support also helped us to maintain the neck length and cancellous graft helped in fracture healing and to some extent improve vascularity of femoral head which made him walk again. Patient may have LLD which is to be addressed at skeletal maturity.
Clinical Relevance
Although fracture neck of femur in children is a rare injury, complications are very common and challenging to treat. Thorough investigations are must before treating these complications of neck of femur fracture. Infection must be ruled out in failed osteosynthesis. In selected cases fibula strut grafting and cancellous grafting allow neck reconstruction and fracture healing without fixation in children. Initial immobilization with spica cast and close follow up and monitoring during post operative period is essential to achieve the goal.
References
1. Miller WE (1973) Fractures of the hip in children from birth to adolescence. Clin Orthop Relat Res 92:155–187 [PubMed]
2. Ratliff AHC (1962) Fractures of the neck of the femur in children. J Bone Joint Surg Br 44:528–542 [PubMed]
3. Chrestian P, Bollini G, Jacquemier M, Ramaherison P (1981) Fractures du col du femur de lénfant. Chir Pediatr 22:397–403 [PubMed]
4. Ratliff AHC (1970) Complications after fractures of the femoral neck in children and their treatment. J Bone Joint Surg Br 52:175–183 .
5. Delbet cited by Colonna PC (1929) Fractures of the neck of the femur in children. Am J Surg 6:793–797.
6. RatliffAHC (1962) Fractures of the neck of the femur in children. J Bone Joint Surg Br 44:528–542[PubMed]
7. Pedro F. Tucci Neto, Fernando Baldy dos Reis, José Laredo Filho, , Edison Noboru Fujiki,Henri Bensahel, and Carlo Milani; Nonunion of fractures of the femoral neck in children ;J Child Orthop. 2008 Mar; 2(2): 97–103.
8. Amit Roshan, , The Neglected Femoral Neck Fracture in Young Adults: Review of a Challenging Problem; Clin Med Res. 2008 May; 6(1): 33–39.
9. Nagi ON, Dhillon MS, Gill SS.Fibular osteosynthesis for delayed type II and type III femoral neck fractures in children.J Orthop Trauma. 1992;6(3):306-13.
10. Miller WE (1973) Fractures of the hip in children from birth to adolescence. Clin Orthop Relat Res 92:155–187 [PubMed]
11. Rang M (1983) Children’s fractures. 2nd edn. J B Lippincott, Philadelphia
12. Canale ST, Bourland WL (1977) Fracture of the neck of the femur and intertrochanteric region of the femur in children. J Bone Joint Surg Am 59:431–443 [PubMed]
13. Ingram AJ, Bachynski B (1953) Fractures of the hip in children. J Bone Joint Surg Am 35:867–886[PubMed]
14. Lam SF (1971) Fractures of the neck of the femur in children. J Bone Joint Surg Am 53:1165–1179[PubMed]
15. Forlin E, Guille BA, Kumar SJ, Rhee KJ (1992) Complications associated with fracture of the neck of the femur in children. J Pediatr Orthop 12:503–509 [PubMed]
16. Hughes LO, Beaty JH (1994) Fractures of the head and neck of the femur in children. J Bone Joint Surg Am 76:283–291 [PubMed]
17. Colonna PC (1928) Fracture of the neck of the femur in childhood. Ann Surg 88:902–907[PMC free article] [PubMed]
18. Weiner DS, O’dell HW (1969) Fractures of the hip in children. J Trauma 9:62–79 [PubMed]
19. Durbin FC (1959) Avascular necrosis complicating undisplaced fractures of the neck of the femur in children. J Bone Joint Surg Br 41:758–765 [PubMed]
20. McDougall A (1961) Fractures of the neck of the femur in childhood. J Bone Joint Surg Br 43:16–28
21. Ogden JA (1974) Changing patterns of proximal femoral vascularity. J Bone Joint Surg Am 56:941–50[PubMed]
22. Trueta J (1957) The normal vascular anatomy of the human femoral head during growth. J Bone Joint Surg Br 39:358–373 [PubMed]
23. Chung SMK (1976) The arterial supply of the developing proximal end of the human femur. J Bone J Surg Am 58:961–970 [PubMed]
24. Sotto-Hall R, Johnson LH, Johnson RA (1964) Variations in the intra-articular pressure of the hip joint in injury and disease. J Bone Joint Surg Am 46:509–516 [PubMed]
25. Drake JK, Meyers MH (1984) Intracapsular pressure and hemartrosis following femoral neck fracture. Clin Orthop Relat Res 182:172–175 [PubMed]
26. Pauwels F (1965) Biomechanics of the locomotor apparatus. English edn. Springer, New York
27. Touzet P, Rigault P, Padovani JP, Pouliquen JC, Mallet JF, Guyonvarch G (1979) Fractures of the neck of the femur in children. Rev Chir Orthop Reparatrice Appar Mot 65:341–349 [PubMed]
28. Trueta J (1968) Vascular pattern of the femoral head during growth. In: Studies of the development decay of the human frame, 2nd ed. J. B. Lippincott, Philadelphia.
| How to Cite this Article: Kumar EGM, Kumar GMY. Osteosynthesis in a 10 year old boy with fracture neck of femur, infected nonunion with implants insitu, neck resorption and Avascular Necrosis -A case report. International Journal of Paediatric Orthopaedics July-Sep 2015;1(1):48-50. |