
License
![]()
International Journal of Paediatric Orthopaedics is licensed under a
https://creativecommons.org/licenses/by-nc-sa/4.0/
Publisher
Official Journal of:
Paediatric Orthopaedic Society of India (POSI)
Publisher:
ResearchOne Publishing House,
An "Indian Orthopaedic Research Group (IORG) initiative.
IORG House,
A-203, Manthan Apts, Shreesh CHS, Hajuri Road,
Thane [West], Maharashtra, India.
Pin Code- 400604
Tel- 02225834545
Publisher Email: indian.ortho@gmail.com
Editor Email: editor.ijpo@gmail.com
pwktoto
holyslot123
Amanah99
Rupiah777
horastogel
cuanslot
okta138
tango168
lotus777
bostoto138
medali69
milojitu
Lotre78
lux77
Gorilatoto
Hoki338
Dewapoker77
baikbet
sule78
lavatoto
uang138
Merak99
porto4d
hemattoto
Kaca138
puri138
anginbet
Joglo4d
juragantogel
Mahyong69
sojubet
sakti777
StarJoker69
grab78
spacetogel
jarum169
Kudatoto
pangkalanbet
ten88
opera99
satelit69
koin88
pondok338
jaring338
pubtogel
milo338
thor388
deltatoto
bdjitu
mirana99
amat123
autobet123
Shio77
gemoy188
planet888
Maria99
makmurwin
pakdejp
geber777
lato777
Melatibet
bankslot
hujantogel
coco69
Rusa69
Apollo303
sule777
namabet
Mars77
moon138
Pancingslot
Pulaubet
rumah88
cumi303
prada68
versace138
Koala4d
lobby69
lux78
usaha4d
kambingtogel
Musangtoto
delta777
Jeweltoto
pos188
lava77
maluku303
kompor88
luckslot
Lotre169
lotus68
raffi169
tambang388
ratuzeusqq
dinasti99
Modalhoki108
asiajitu
judi78
astra78
partaiqq
rumah69
Meriam123
evosbet88
Sayangbet
Lilin4d
Cemaraslot
furla69
kumis4d
Bandungslot
japan78
hokislot123
hulk303
Pragmatic69
chivas69
krisna188
Lyonslot
ASIABET168
topislot
bola123
ultra365
ios55
kompor77
sinaga138
kelapabet
padang777
Rajawin777
Jakarta88slot
Becak168
babetogel
primaslot
Moonslot
palu338
pulautogel
botaktogel
platinum138
cici169
gunturtogel
Kacang4d
dewabet138
spin388
homebet69
bursatoto
mami4d
pasbet
aduhoki
lava69
pagoda388
meledak99
dalang138
Gama188
dino777
papua338
darat123
hokiwin55
Cobra777
Merak88
crown78
preman77
grab188
terminal388
apiwin
madura78
sinar303
Dupawin
Santuy188
kera388
Modalhoki68
omuslot
Peri123
divabet
macau388
Angsa138
keris69
DOMINOPKV
Bos69
Sawitjitu
jaring99
layar77
tayototo
taro168
pejuang388
next88
harapan168
hemat123
Shio88
apidewa77
parisjp
pohon69
Lotre777
taruna123
asean168
giga69
StarJoker123
tempat99
Sisir4d
Tokek78
bosstogel
pakdeslot88
wisslot
rumah108
dominoslot
cola123
jili88
kompas77
bisnis77
kungfu69
Arjuna77
sensa123
Piramida4d
gacor365
pucuk777
Lotre123
wayang777
Gama178
WLA88
langitmpo
Robot4d
kumbang123
Logam4d
Sawit138
Bca168
petir88
tokyobet
tempo123
Permen178
Gacorbos99
wiratogel
LUNAS805
sateslot
barbar188
maxwin123
pecahtogel
Menang77
demotogel
trisula4d
candy138
bostoto188
demo388
citatogel
SIRKUIT138
Boy4d
Kalaslot
formulabet
Kode99
icon55
domino123
cartel303
jingga4d
Luxuryqq
space168
Legenda4d
porto169
api69
ASIAMPO77
wiki69
fasslot
cincin77
rajatoto68
Merak78
batastogel
gem108
buku99
furlabet
versace168
Sayang777
marvel365
kumis138
sushitoto
cbototo
latar77
Hadiah4d
solusi138
udara4d
sayang188
maha777
milo55
taro303
Dunia88
sejuta188
Dewapokertogel
Luxurygg
KOBOYPOKER
Aksara77
amat303
unggul123
oris77
kingdomjitu
merci4d
Aontoto
gemoyslot
geloratoto
layar69
winning138
sobet78
klik303
gilagg
bantamtoto
Sbo4d
Tombol4d
maya303
spin6d
sumo123
lambe88
barbar88
kadobet168
solid169
oasis365
karo303
duta69
sumo88
Pandawa123
ipar777
bengkelslot
macanslot
abc69
judolbetqq
Laku123
obor77
Lampion4d
memori77
jepang169
plntoto
ASIAPKV
Duyung88
Hijau123
dewanslot
MAXWIN888
SUARABET77
empirebet
Kucingtoto
kakek138
idr188
coca123
sisri77
jamu123
cumi99
fire123
persentogel
moon4d
dutabet
jaring365
Bigwin178
Gacorbos169
toto388
evosgamingg
kado99
WLA55
kadal303
rumah168
Poker138
Aztectoto
gasing78
extrabet
urban168
Topengslot
planet388
Angkatoto77
mulia88
qq69
luck388
epictogel
GACORBOS
icon169
atlas169
bentototo
jamu4d
libas169
holiday69
hulk77
skor77
karo168
colekbet
Bendera99
suhu4d
Dayak123
radentogel
KOBOY888
memori108
lajubet888
JUARAWIN88
BIMO77
jokerbetqq
AREASLOTO
juara77
dewi138
DEWIBET777
nusapoker
jilibet
Ikan303
kadalslot
depototo
harum123
pawang88
krisna123
madu55
Khusustogel
taktik388
Wahana4d
ovo168
mesinslot
Gogo90
bromo99
Badutjitu
Mega777
sentosa69
kamus168
Tigerslot
tempatslot
wazebet
sekai777
airtogel
Agen99
colek777
pasang388
pigi388
Angkatoto123
batam69
kudetabet69
mewah123
fuji338
papua78
murahpoker
cincin365
memori69
hantu78
anak777
Kapten99
Nanas188
Glory77
wiki78
PEDANGBET
mahjongs138
ipar78
motoslot88
POV99
bingo4d
ratuslot777
YUPI188
ASIASLOT888
fire777
pasti138
batam777
julietslot
iklan88
kamus77
sobet99
capital99
Sicbo4d
paris4d
daya365
amat168
roslot55
Kaktusslot
cakra123
Abu123
krisna77
guntur365
PEDANGJITU
panca123
Kodok123
ASIAKING777
JPSLOT168
wuling88
kaya77
KOBOIBOLA
garpu777
kingbet169
pir69
extra188
oren77
cair365
kingdomjp
dewaslot138
nagapoker777
cici138
Daun777
surga6d
holyslottoto
jakarta303
dinasti777
suara78
Mbah4d
HOKIOM88
zona77
unggul169
tempat123
Arus138
retro388
mampirtoto
sulaptogel
nagawin168
pecah188
bangsa338
ASIAHOKI88
neopoker
mesin188
canduslot777
dino78
asus88
Mangga4d
kumistogel
nama88
kkslot55
LUNA999
Tokcer69
Logam303
kkslot108
lgo188
gemoy777
ultra99
tahunslot
ligajp88
kampusslot
babe69
macau128
taktik123
kado338
Angsa77
latarslot
juliet777
lavaslot
suburbet
doyan77
ladang77
Dupaslot
YUPIBET
AREA188
betagg
usaha169
AREAWIN88
megawinbet
Tokcer168
mandiri99
MANTAP138
mahal99
Gobertogel
abc77
mulia99
bonus303
kembar388
sensatogel
atom188
gebyar77
baik388
balon138
Master77
ovo338
gaco169
edanbet
pistolslot
air169
kembang169
dna303
wigo123
ladangslot
pasang338
suryatogel
DOMINOBET77
kembar188
diva388
pohonjitu
Sakuraqq
kumis168
ASIATOTO777
Premium188
rupiah4d
CERIAPOKER
KAYA78
kebunbet
sawi69
pub365
pesiar69
Wild777
Tores777
paus168
bom108
Dollarjitu
vegas77
wis338
Kancil69
angkasaslot
Dolan138
semangat303
jaritogel
daun69
nova123
darat303
SERUBET88
selat123
hantu88
serbatoto
balon123
tenbet
padi78
benuawin
Sensa188
Emas88
Rajawalitogel
musangtogel
sarana78
sugar365
lexus108
bom123
kso123
luck4d
puncak88
vista123
muara69
Rutantoto
ceria88
RAFI777
alasbet
durentoto
mpomaster
cipitbet
usaha138
leobet
mantra168
Akun188
Nanastogel
alexa88
Tombol168
slotbom68
solid78
gunturslot
sake138
Gloryslot
luck77
raksasa138
mildbet
Doku123
Yakuza777
bostoto77
jutawan168
odin123
lampu168
cumi168
mega169
puri188
petatogel
dadu168
mahadewa168
karirtogel
istana88
serbu123
kumbang99
pulau169
Sarangslot88
muliaslot
tiktoktoto
retro4d
ayo68
Dugem88
jepe338
bns99
leo303
turbo77
timur77
baiktogel
masterbet123
Mansionslot
petirslot
retro69
unggul168
POV69
musik168
kapaljudi777
Habanero138
marvel188
kejubet
ios99
Ninjaslot
permen169
fix338
koi138
madura168
gerbang338
desa77
sushi168
Ikanslot
opera123
oren365
luckbet
Rusa77
Ungu77
hugo99
medan123
zodiaktoto
papua168
mansion88
luck99
asean188
rajazeus138
seru78
kampung99
Target99
gas123
coca4d
dinastibet
sultanbet188
Alamtoto
pwktoto pwktoto
rajagaming-52
rajagaming-53
rajagaming-54
rajagaming-55
rajagaming-56
rajagaming-57
rajagaming-58
rajagaming-59
rajagaming-6
rajagaming-60
rajagaming-61
rajagaming-62
rajagaming-63
rajagaming-64
rajagaming-65
rajagaming-66
rajagaming-67
rajagaming-68
rajagaming-69
rajagaming-7
rajagaming-70
rajagaming-71
rajagaming-72
rajagaming-73
rajagaming-74
rajagaming-75
rajagaming-76
rajagaming-77
rajagaming-78
rajagaming-79
rajagaming-8
rajagaming-80
rajagaming-81
rajagaming-82
rajagaming-83
rajagaming-84
rajagaming-85
rajagaming-86
rajagaming-87
rajagaming-88
rajagaming-89
rajagaming-9
rajagaming-90
rajagaming-91
rajagaming-92
rajagaming-93
rajagaming-94
rajagaming-95
rajagaming-96
rajagaming-97
rajagaming-98
rajagaming-99
sibayak99
triadtotogroup
nagatoto88
garwa4d
Kirintoto
triadsgp
triadsyd
triadjitu
triadmacau
triadtoto
triadtogel
triad4d
triadhk
torpedo99
scatter99
boom138
bosslot138
sibayak99
emas69
triad303
triadslot
pwktoto
triadtogel
triadhk
nagatoto88
garwa4d
torpedo4d
triadmacau
triadtoto
triadmacau
triadtoto
triadtogel
triadhk
scatter99
sibayak99
emas69
triadjitu
emas69
scatter99
sibayak99
boom138
pwktoto
torpedo4d
torpedo4d
torpedo4d
torpedo4d
nagatoto88
nagatoto88
nagatoto88
garwa4d
garwa4d
garwa4d
triadtoto
triadtoto
triadtoto
triadtogel
triadtogel
triadtogel
triad4d
triad4d
triad4d
triad4d
triad4d
triad4d
triadhk
triadhk
triadhk
triadhk
triadhk
triadhk
triadmacau
triadmacau
triadjitu
triadjitu
triadjitu
scatter99
scatter99
scatter99
scatter99
scatter99
sibayak99
sibayak99
sibayak99
sibayak99
sibayak99
sibayak99
sibayak99
sibayak99
boom138
emas69
emas69
rokettoto
rokettoto
rokettoto
rokettoto
bukitdita
kirintoto
kirintoto
triadsgp
triadsgp
triadsyd
triadsyd
torpedo99
torpedo99
torpedo99
torpedo99
premium138
premium138
premium138
premium138
premium138
premium138
bosslot138
bosslot138
bosslot
bosslot138
bosslot138
pusat69
pusat69
dompet69
dompet69
dompet69
dompet138
dompet188
dompet168
dompet123
harta69
triadslot
triadslot
triad303
138vip
138vip
triadtogel
triadtoto
triad4d
triadhk
triadhk
triad4d
triadtogel
triadjitu
triadmacau
boom138
garwa4d
scatter99
emas69
torpedo4d
nagatoto88
vinaslot
vinaslot
vinaslot
pwktoto
holyslot123
Amanah99
Rupiah777
horastogel
cuanslot
okta138
tango168
lotus777
bostoto138
medali69
milojitu
Lotre78
lux77
Gorilatoto
Hoki338
Dewapoker77
baikbet
sule78
lavatoto
uang138
Merak99
porto4d
hemattoto
Kaca138
puri138
anginbet
Joglo4d
juragantogel
Mahyong69
sojubet
sakti777
StarJoker69
grab78
spacetogel
jarum169
Kudatoto
pangkalanbet
ten88
opera99
satelit69
koin88
pondok338
jaring338
pubtogel
milo338
thor388
deltatoto
bdjitu
mirana99
amat123
autobet123
Shio77
gemoy188
planet888
Maria99
makmurwin
pakdejp
geber777
lato777
Melatibet
bankslot
hujantogel
coco69
Rusa69
Apollo303
sule777
namabet
Mars77
moon138
Pancingslot
Pulaubet
rumah88
cumi303
prada68
versace138
Koala4d
lobby69
lux78
usaha4d
kambingtogel
Musangtoto
delta777
Jeweltoto
pos188
lava77
maluku303
kompor88
luckslot
Lotre169
lotus68
raffi169
tambang388
ratuzeusqq
dinasti99
Modalhoki108
asiajitu
judi78
astra78
partaiqq
rumah69
Meriam123
evosbet88
Sayangbet
Lilin4d
Cemaraslot
furla69
kumis4d
Bandungslot
japan78
hokislot123
hulk303
Pragmatic69
chivas69
krisna188
Lyonslot
ASIABET168
topislot
bola123
ultra365
ios55
kompor77
sinaga138
kelapabet
padang777
Rajawin777
Jakarta88slot
Becak168
babetogel
primaslot
Moonslot
palu338
pulautogel
botaktogel
platinum138
cici169
gunturtogel
Kacang4d
dewabet138
spin388
homebet69
bursatoto
mami4d
pasbet
aduhoki
lava69
pagoda388
meledak99
dalang138
Gama188
dino777
papua338
darat123
hokiwin55
Cobra777
Merak88
crown78
preman77
grab188
terminal388
apiwin
madura78
sinar303
Dupawin
Santuy188
kera388
Modalhoki68
omuslot
Peri123
divabet
macau388
Angsa138
keris69
DOMINOPKV
Bos69
Sawitjitu
jaring99
layar77
tayototo
taro168
pejuang388
next88
harapan168
hemat123
Shio88
apidewa77
parisjp
pohon69
Lotre777
taruna123
asean168
giga69
StarJoker123
tempat99
Sisir4d
Tokek78
bosstogel
pakdeslot88
wisslot
rumah108
dominoslot
cola123
jili88
kompas77
bisnis77
kungfu69
Arjuna77
sensa123
Piramida4d
gacor365
pucuk777
Lotre123
wayang777
Gama178
WLA88
langitmpo
Robot4d
kumbang123
Logam4d
Sawit138
Bca168
petir88
tokyobet
tempo123
Permen178
Gacorbos99
wiratogel
LUNAS805
sateslot
barbar188
maxwin123
pecahtogel
Menang77
demotogel
trisula4d
candy138
bostoto188
demo388
citatogel
SIRKUIT138
Boy4d
Kalaslot
formulabet
Kode99
icon55
domino123
cartel303
jingga4d
Luxuryqq
space168
Legenda4d
porto169
api69
ASIAMPO77
wiki69
fasslot
cincin77
rajatoto68
Merak78
batastogel
gem108
buku99
furlabet
versace168
Sayang777
marvel365
kumis138
sushitoto
cbototo
latar77
Hadiah4d
solusi138
udara4d
sayang188
maha777
milo55
taro303
Dunia88
sejuta188
Dewapokertogel
Luxurygg
KOBOYPOKER
Aksara77
amat303
unggul123
oris77
kingdomjitu
merci4d
Aontoto
gemoyslot
geloratoto
layar69
winning138
sobet78
klik303
gilagg
bantamtoto
Sbo4d
Tombol4d
maya303
spin6d
sumo123
lambe88
barbar88
kadobet168
solid169
oasis365
karo303
duta69
sumo88
Pandawa123
ipar777
bengkelslot
macanslot
abc69
judolbetqq
Laku123
obor77
Lampion4d
memori77
jepang169
plntoto
ASIAPKV
Duyung88
Hijau123
dewanslot
MAXWIN888
SUARABET77
empirebet
Kucingtoto
kakek138
idr188
coca123
sisri77
jamu123
cumi99
fire123
persentogel
moon4d
dutabet
jaring365
Bigwin178
Gacorbos169
toto388
evosgamingg
kado99
WLA55
kadal303
rumah168
Poker138
Aztectoto
gasing78
extrabet
urban168
Topengslot
planet388
Angkatoto77
mulia88
qq69
luck388
epictogel
GACORBOS
icon169
atlas169
bentototo
jamu4d
libas169
holiday69
hulk77
skor77
karo168
colekbet
Bendera99
suhu4d
Dayak123
radentogel
KOBOY888
memori108
lajubet888
JUARAWIN88
BIMO77
jokerbetqq
AREASLOTO
juara77
dewi138
DEWIBET777
nusapoker
jilibet
Ikan303
kadalslot
depototo
harum123
pawang88
krisna123
madu55
Khusustogel
taktik388
Wahana4d
ovo168
mesinslot
Gogo90
bromo99
Badutjitu
Mega777
sentosa69
kamus168
Tigerslot
tempatslot
wazebet
sekai777
airtogel
Agen99
colek777
pasang388
pigi388
Angkatoto123
batam69
kudetabet69
mewah123
fuji338
papua78
murahpoker
cincin365
memori69
hantu78
anak777
Kapten99
Nanas188
Glory77
wiki78
PEDANGBET
mahjongs138
ipar78
motoslot88
POV99
bingo4d
ratuslot777
YUPI188
ASIASLOT888
fire777
pasti138
batam777
julietslot
iklan88
kamus77
sobet99
capital99
Sicbo4d
paris4d
daya365
amat168
roslot55
Kaktusslot
cakra123
Abu123
krisna77
guntur365
PEDANGJITU
panca123
Kodok123
ASIAKING777
JPSLOT168
wuling88
kaya77
KOBOIBOLA
garpu777
kingbet169
pir69
extra188
oren77
cair365
kingdomjp
dewaslot138
nagapoker777
cici138
Daun777
surga6d
holyslottoto
jakarta303
dinasti777
suara78
Mbah4d
HOKIOM88
zona77
unggul169
tempat123
Arus138
retro388
mampirtoto
sulaptogel
nagawin168
pecah188
bangsa338
ASIAHOKI88
neopoker
mesin188
canduslot777
dino78
asus88
Mangga4d
kumistogel
nama88
kkslot55
LUNA999
Tokcer69
Logam303
kkslot108
lgo188
gemoy777
ultra99
tahunslot
ligajp88
kampusslot
babe69
macau128
taktik123
kado338
Angsa77
latarslot
juliet777
lavaslot
suburbet
doyan77
ladang77
Dupaslot
YUPIBET
AREA188
betagg
usaha169
AREAWIN88
megawinbet
Tokcer168
mandiri99
MANTAP138
mahal99
Gobertogel
abc77
mulia99
bonus303
kembar388
sensatogel
atom188
gebyar77
baik388
balon138
Master77
ovo338
gaco169
edanbet
pistolslot
air169
kembang169
dna303
wigo123
ladangslot
pasang338
suryatogel
DOMINOBET77
kembar188
diva388
pohonjitu
Sakuraqq
kumis168
ASIATOTO777
Premium188
rupiah4d
CERIAPOKER
KAYA78
kebunbet
sawi69
pub365
pesiar69
Wild777
Tores777
paus168
bom108
Dollarjitu
vegas77
wis338
Kancil69
angkasaslot
Dolan138
semangat303
jaritogel
daun69
nova123
darat303
SERUBET88
selat123
hantu88
serbatoto
balon123
tenbet
padi78
benuawin
Sensa188
Emas88
Rajawalitogel
musangtogel
sarana78
sugar365
lexus108
bom123
kso123
luck4d
puncak88
vista123
muara69
Rutantoto
ceria88
RAFI777
alasbet
durentoto
mpomaster
cipitbet
usaha138
leobet
mantra168
Akun188
Nanastogel
alexa88
Tombol168
slotbom68
solid78
gunturslot
sake138
Gloryslot
luck77
raksasa138
mildbet
Doku123
Yakuza777
bostoto77
jutawan168
odin123
lampu168
cumi168
mega169
puri188
petatogel
dadu168
mahadewa168
karirtogel
istana88
serbu123
kumbang99
pulau169
Sarangslot88
muliaslot
tiktoktoto
retro4d
ayo68
Dugem88
jepe338
bns99
leo303
turbo77
timur77
baiktogel
masterbet123
Mansionslot
petirslot
retro69
unggul168
POV69
musik168
kapaljudi777
Habanero138
marvel188
kejubet
ios99
Ninjaslot
permen169
fix338
koi138
madura168
gerbang338
desa77
sushi168
Ikanslot
opera123
oren365
luckbet
Rusa77
Ungu77
hugo99
medan123
zodiaktoto
papua168
mansion88
luck99
asean188
rajazeus138
seru78
kampung99
Target99
gas123
coca4d
dinastibet
sultanbet188
Alamtoto
pwktoto pwktoto
rajagaming-52
rajagaming-53
rajagaming-54
rajagaming-55
rajagaming-56
rajagaming-57
rajagaming-58
rajagaming-59
rajagaming-6
rajagaming-60
rajagaming-61
rajagaming-62
rajagaming-63
rajagaming-64
rajagaming-65
rajagaming-66
rajagaming-67
rajagaming-68
rajagaming-69
rajagaming-7
rajagaming-70
rajagaming-71
rajagaming-72
rajagaming-73
rajagaming-74
rajagaming-75
rajagaming-76
rajagaming-77
rajagaming-78
rajagaming-79
rajagaming-8
rajagaming-80
rajagaming-81
rajagaming-82
rajagaming-83
rajagaming-84
rajagaming-85
rajagaming-86
rajagaming-87
rajagaming-88
rajagaming-89
rajagaming-9
rajagaming-90
rajagaming-91
rajagaming-92
rajagaming-93
rajagaming-94
rajagaming-95
rajagaming-96
rajagaming-97
rajagaming-98
rajagaming-99
sibayak99
triadtotogroup
nagatoto88
garwa4d
Kirintoto
triadsgp
triadsyd
triadjitu
triadmacau
triadtoto
triadtogel
triad4d
triadhk
torpedo99
scatter99
boom138
bosslot138
sibayak99
emas69
triad303
triadslot
pwktoto
triadtogel
triadhk
nagatoto88
garwa4d
torpedo4d
triadmacau
triadtoto
triadmacau
triadtoto
triadtogel
triadhk
scatter99
sibayak99
emas69
triadjitu
emas69
scatter99
sibayak99
boom138
pwktoto
torpedo4d
torpedo4d
torpedo4d
torpedo4d
nagatoto88
nagatoto88
nagatoto88
garwa4d
garwa4d
garwa4d
triadtoto
triadtoto
triadtoto
triadtogel
triadtogel
triadtogel
triad4d
triad4d
triad4d
triad4d
triad4d
triad4d
triadhk
triadhk
triadhk
triadhk
triadhk
triadhk
triadmacau
triadmacau
triadjitu
triadjitu
triadjitu
scatter99
scatter99
scatter99
scatter99
scatter99
sibayak99
sibayak99
sibayak99
sibayak99
sibayak99
sibayak99
sibayak99
sibayak99
boom138
emas69
emas69
rokettoto
rokettoto
rokettoto
rokettoto
bukitdita
kirintoto
kirintoto
triadsgp
triadsgp
triadsyd
triadsyd
torpedo99
torpedo99
torpedo99
torpedo99
premium138
premium138
premium138
premium138
premium138
premium138
bosslot138
bosslot138
bosslot
bosslot138
bosslot138
pusat69
pusat69
dompet69
dompet69
dompet69
dompet138
dompet188
dompet168
dompet123
harta69
triadslot
triadslot
triad303
138vip
138vip
triadtogel
triadtoto
triad4d
triadhk
triadhk
triad4d
triadtogel
triadjitu
triadmacau
boom138
garwa4d
scatter99
emas69
torpedo4d
nagatoto88
vinaslot
vinaslot
vinaslot
pwktoto

Neglected clubfoot: Patho-anatomy and clinical features
Volume 2 | Issue 1 | Jan-Apr 2016 | Page 2-5|Mandar Agashe
Authors : Mandar Agashe [1*]
Director, Centre for Paediatric Orthopaedic Care (CPOC) at Dr. Agashe’s Hospital, Kurla, Maharashtra, India
Address of Correspondence
Dr Mandar Agashe
Centre for Paediatric Orthopaedic Care (CPOC) at Dr. Agashe’s Hospital, Kurla, Mumbai, India.
Email: mandarortho@gmail.com
Abstract
Neglected clubfoot still remains a great problem in developing countries like India especially in the rural population with limited access to modern healthcare. It is the most common congenital problem leading to locomotor disability, so much so that the government of India has, in recent years added congenital clubfoot in one the eight notifiable conditions at birth with the hope of eliminating the scrouge of neglected clubfoot. With the popularity of the Ponseti method, more and more cases of congenital clubfoot are being treated at the time when they should be ideally treated- ie neonatal period and early infancy. However there are still some lacunae in the healthcare delivery system in India, leading to persistence of these neglected cases in rural population. The obstacles of poverty, lack of awareness and lack of medical facilities in accessible locations means that treatment is either not initiated or incompletely performed.
Since the deformity in neglected cases is a complex three-dimensional one, it is essential to understand the pathoanatomy of the same before embarking on the treatment. In this article, we deal with the detailed pathoanatomy as well as the clinical features related to neglected clubfeet.
Keywords: Congenital talipes equino varus, clubfeet, neglected
Introduction:
Neglected clubfoot still remains a great problem in developing countries like India especially in the rural population with limited access to modern healthcare[1,2]. It is the most common congenital problem leading to locomotor disability, so much so that the government of India has, in recent years added congenital clubfoot in one the eight notifiable conditions at birth with the hope of eliminating the scrouge of neglected clubfoot. With the popularity of the Ponseti method, more and more cases of congenital clubfoot are being treated at the time when they should be ideally treated- ie neonatal period and early infancy[1]. However there are still some lacunae in the healthcare delivery system in India, leading to persistence of these neglected cases in rural population. The obstacles of poverty, lack of awareness and lack of medical facilities in accessible locations means that treatment is either not initiated or incompletely performed[3,4].
Since the deformity in neglected cases is a complex three-dimensional one, it is essential to understand the pathoanatomy of the same before embarking on the treatment. In this article, we deal with the detailed pathoanatomy as well as the clinical features related to neglected clubfeet.
Pathoanatomy
The pathological anatomy of the neglected clubfoot can be divided into that related to bone and joints and that related to soft tissues (ligaments, muscles and tendons).
Bones and joints[5,6] [Figures 1,2,3]
The talus is the bone which is most affected in neglected clubfoot [blue arrow]. The talus is severely plantarflexed. The body is small and altered in shape. The talus becomes severely inverted in the ankle mortice. The trochlea is shorter than normal. Only the posterior portion of the talus articulates with the tibia in the ankle joint while the anterior portion is just covered with thin and stretched out ankle joint capsule. Normally, the posterior-most portion of the talus is extra-articular. However in neglected clubfeet with severe planter-flexion, the posterior portion of the talus becomes intra-articular and is covered by joint capsule. The neck of the talus develops significant medial angulation and the head becomes wedge shaped. There are two surfaces of the talus- the anterolateral and anteromedial. The anterolateral surface of the talus is left uncovered by the medially displaced navicular and is now covered by just thin joint capsule which is stretched out, and the skin. This is the part which is palpable just underneath the skin. The anteromedial surface now articulates with the navicular which is displaced medially and proximally.
The navicular is also very severely affected in neglected clubfeet [white arrow]. It is flattened or wedge-shaped and medially displaced, adducted and inverted. It articulates with the anteromedial surface of the talus and in some severe cases, even has a pseudo-articulation with the medial malleolus. The enlarged tibialis posterior is attached to a wide area on the navicular along with the medial malleolus.
The calcaneus also undergoes a significant alteration [black arrow]. The body of the calcaneus is severely plantarflexed and medially bowed. It is adducted and the lateral process of the calcaneum is under the talus, rather than being lateral to it. In severe neglected cases, the body of the calcaneus also undergoes severe changes, leading to it being bean-shaped rather than rectangular on the axial plane. The axes of the calcaneum and talus are parallel to each other. The cuboid is also medially displaced at the calcaneo-cuboid joint so that only the medial surface of the anterior process of the calcaneum articulates with the cuboid.
The cuneiforms and metatarsals also undergo secondary changes though to a lesser extent than the talus, calcaneum and navicular. The cuneiforms are medially displaced and have very haphazard articulations with the navicular and the cuboid. The metatarsals are shortened.
The talonavicular joint is entirely medially displaced. This articulation is between the anteromedial surface of the talus and the proximal surface of the navicular. There develop pseudoarticulations between the navicular and the tibia (at the medial malleolus) and also between the navicular and the calcaneum. In some cases, there is a fibrous band which is formed between the navicular and the calcaneum, almost like a fibrous calcaneonavicular bar.
The three talcalcaneal joints (anterior, middle and posterior) are also very abnormal. The anterior facet remains very narrow while the middle facet is variable. The posterior facet is short. The sustentaculum tali is left uncovered to a large extent. In very severe neglected clubfeet, the talo-calcaneal joints are almost in the weight bearing axis due to the severe inversion so that the talus assumes the weightbearing position.
The calcaneocuboid joint orientation is very important for the treatment of neglected clubfeet. The calcaneocuboid joint is very obliquely placed with the cuboid being subluxed anteriorly and medially while the lateral aspect of the calcaneum is left uncovered. The other joints of the foot (ie the intercuneiforms and intermetatarsals) follow the course of the main joints of the midfoot and hindfoot. The point to remember is that the first two metatarsals are severely pronated while the lateral three metatarsals are supinated. The degree of pronation will determine the cavus, which in turn will determine the fate of the foot in terms of whether the child walks on the lateral border or the dorsal surface.
Pathoanatomy of soft tissues (ligaments, muscles and tendons)[5-7]
The soft tissues in clubfeet also undergo a significant amount of secondary changes. They are subclassified as:
1) Changes in muscles:
The triceps surae and the tendoachilles is the most severely affected amongst all muscle tendon units in neglected clubfeet. The severity of neglected clubfoot depends mainly on the amount of shortening of the tendoachilles.Both the triceps surae and the tendoachilles are foreshortened and the tendon is significantly longer than the muscle. The tendoachilles is inserted medially on the calcaneus and is one of the deforming forces to pull the heel in varus.
Amongst the other muscle tendon units affected, the tibialis posterior is very important. The tibialis posterior becomes very broad and hypertrophied and is inserted over a very broad area on the inferomedial surface of the navicular and the medial cuneiform. This is the most important cause of supination of the foot. In some very severe cases, the tibialis posterior also seems to have an additional thick fibrous band which is attached to the cuboid, which pulls the cuboid medially. This itself leads to the significant displacement of the calcaneocuboid joint, which is seen in some cases.
The tibialis anterior undergoes some amount of hypertrophy. This is more apparently seen in incompletely treated clubfeet, in which the tibialis anterior causes a dynamic supination deformity during the swing phase of gait. The other muscles of the flexor compartment of the foot also undergo foreshortening with resultant clawing.
2) Changes in ligaments and other soft tissues:
The plantar fascia is very tight and results in the cavus component of the deformity. The amount of tightness of the plantar fascia and the cavus, decide how the child walks in neglected clubfeet[4-6]. If the cavus is moderately severe, the child walks on the lateral border of the foot. However if the cavus is exceedingly severe, the child starts walking on the dorsal surface of the foot, making normal ambulation exceedingly difficult.
In the ligaments, the deep layer of the deltoid ligament is very thick and forms a part of the pseudoarticulation between the medial malleolus and the medially displaced navicular. The tibianavicular and the calcaneonavicular ligaments are thickened and shortened. The ligaments on the medial, plantar and the posterior aspect of the foot undergo severe thickening with shortening and are the main tethers against effective closed manipulative treatment of neglected feet. Amongst them, the medial talo-calcaneal ligament and the plantar calcaneonavicular ligaments are very important. The eponymous “knot of Henry” becomes a thick fibrous band which extends from the undersurface of the navicular till the plantar surface of the medial cuneiform and the talus in neglected clubfeet.
Thus to conclude, neglected clubfoot is a three dimensional deformity, with severe secondary changes in bones, muscles, tendons and ligaments, all of whom have to be corrected for effective clinical management.
Clinical features
The neglected clubfoot, by definition is a foot which has experienced no or minimal surgical or non-surgical management[6] [figure 4]. In this case, the deformity starts increasing after the child starts weightbearing. This is because the structures which are never meant to bear the weight of the body are now in a weight bearing position, the weightbearing starts happening on the side and dorsum of the foot and secondary contractures start developing on the plantar-medial and posterior side of the foot. There is usually a large bursa or callosity at the lateral aspect of the foot, which on prolonged weight-bearing leads to skin breakdowns, ulcerations and infections. It is often difficult or impossible to wear normal shoes for ambulation.
Patterns of deformity[6]
Just like clubfoot deformity in the neonatal and infantile period, there are different patterns of deformity in a neglected clubfoot. Though all the major components of the deformity, ie cavus, forefoot adductus, heel varus and equinus are present in all patients, the exact combination is the main causative factor for a particular type of deformity. As a result, there are various feet with different grades of stiffness, mobility and deformity. This led a few investigators to subclassifiy the deformities in neglected clubfeet into three patterns of deformity since the treatment modality followed and prognosis depends on each of these patterns.
1) Moderately flexible: The foot can be considerably corrected to neutral position
2) Moderately stiff: There is some correctability but not to neutral position and with moderate deformity persisting
3) Rigid: There is almost no correction of deformity.
The classification can be applied either to the entire foot, or separately to the midfoot and hindfoot. Of course, the standard classifications of Pirani[8] and Dimeglio[9] can still be used additionally.
As explained previously, the degree of cavus determines whether the child walks on the lateral border of the foot or the dorsum of the foot. In lesser degree of cavus, the child walks on the lateral border while in greater degree of cavus the child walks on the dorsal surface itself. In the presence of this severe cavus, it is very difficult to appreciate the amount of equinus actually present. This usually gets unmasked once the cavus and adductus gets corrected.
Socio-economic factors
The kids with neglected clubfeet eventually learn to walk with no or some modified footwear[6]. However, it is a condition which is fraught with numerous struggles. This deformity poses a significant disability in young children, preventing access to education and social activity[10]. Many of them are outcast or even deemed as “cursed” with very little social interaction due to the obvious grotesque deformity[6]. Social stigma of having “reverse feet” is also very great, and many girls find it difficult to get married due to this[4]. They are unable to squat for toileting purposes which is an essential function especially in rural population[3,4]. There is significant pain, difficulty in locomotion over long distance, with frequent skin breakdowns, infections and callosities. The skin breakdowns and infections can sometimes be so severe that it may lead to amputations.
Conclusion
Congenital clubfoot is a complex problem which requires proper understanding of the anatomy as well as realistic goals for treatment before embarking on attempting to treat it.
References
1. Gadhok K, Belthur MV, Aroojis AJ, Cook T, Oprescu F, Ranade AS, Morcuende JA. Qualitative assessment of the challenges to the treatment of idiopathic clubfoot by the Ponseti method in urban India. Iowa Orthop J. 2012;32:135-40.
2. Lohia LK, Meena S, Kanojia RK Comparative study of complete subtalar release and Joshi’s external stabilization system in the management of neglected and resistant idiopathic clubfoot..Foot Ankle Surg. 2015 Mar;21(1):16-21.
3. Shingade V, Shingade R, Ughade S Single-stage correction for clubfoot associated With myelomeningocele in older children: early results Curr. Orthop. Practice 2014;25(1),64-70.
4. Shingade V, Shingade R, Ughade S. Correction of neglected or relapsed clubfoot deformity in an older child with single stage procedure: Early results. Curr. Orthop Practice. 2012; 23(2), 122-129.
5. Ponseti IV. Congenital clubfoot: Fundamentals for treatment. Oxford: Oxford University Press: 1996.
6. Penny JN. The neglected clubfoot. Techniques in Orthopaedics Vol 20. Philadelphia: Lippincott Williams & Wilkins Inc.; 2005: 153–166.
7. Scott WA, Hosking SW, Caterall A. Clubfoot. Observations on the surgical anatomy of dorsiflexion. J Bone Joint Surg (Br) 1984;66: 71-6.
8. Pirani S. A reliable and valid method of assessing the amount of deformity in the congenital clubfoot. Presented at the Pediatric Orthopaedic society of North America, May 2004; St. Louis.
9. Demiglio A, Bensahel H, Souchet P, et al. Classification of clubfoot. J Pediatr Orthop (B) 1996;4:129-136.
10. Owen RM, Penny JN, Mayo A, Morcuende J, Lavy CB. A collaborative public health approach to clubfoot intervention in 10 low-income and middle-income countries: 2-year outcomes and lessons learnt. J Pediatr Orthop B. 2012 Jul;21(4):361-5.
11. Sengupta A. The management of congenital talipes equinovarus in developing countries. Int Orthop 1987;11: 183-187.
(Abstract) (Full Text HTML) (Download PDF)
Pink Pulseless hand – Evaluation and Decision making: Is there a Consensus?
Vol 1 | Issue 1 | July-Sep 2015 | page:19-22 | Venkatadass K.
Authors : Venkatadass K[1].
[1] Consultant Paediatric Orthopaedic Surgeon, Ganga Medical Centre & Hospitals, Coimbatore, India.
Address of Correspondence
Dr. K. Venkatadass
Ganga Medical Centre & Hospitals, Coimbatore, India.
Email- venkatpedortho@gmail.com
Abstract
Background: The standard of care for the initial treatment of pulseless supracondylar fracture of the humerus is emergency closed reduction and percutaneous pin stabilization. Some of these patients remain pulseless even after closed reduction and pin fixation with a well perfused hand. The management of this so-called pink pulseless hand still remains controversial. The options described in the literature are either of the two extremes of just observation or exploration of the vessel and vascular repair if needed. There are no clear guidelines on when to explore a pink pulseless hand. This article reviews the current literature on this gray area with recommendations on the process of evaluation and decision-making in pink pulseless hand.
Keywords: Supracondylar humerus fracture, vascular injury, pink pulseless hand.
Introduction
The incidence of vascular injuries associated with displaced supracondylar fractures of humerus in children is about 10-20% [1,2,3]. It is reported to be more common in extension type fractures due to the close proximity of the proximal fragment to the neurovascular bundle [4,5]. In a child presenting with a pulseless supracondylar humerus fracture an urgent closed reduction with percutaneous pin stabilization is recommended. In majority of these patients the injured limb gets back the pulse and the hand appears well perfused after closed reduction and pin fixation. These patients are then treated as any other patient with supracondylar fracture humerus without any additional special precaution [3]. There is no confusion in the literature regarding the management of those patients in whom the limb remains pulseless, pale and unperfused after a closed reduction and stabilization [3]. Emergency exploration of the artery and arterial repair if needed to get back the circulation of the affected limb is the current recommendation. But there is still no consensus on the management of those limbs, which remain pulseless after closed reduction and pinning, but are pink and well perfused. The main reason for this confusion is lack of details of natural history of this entity [2]. The current literature on this enigmatous situation has been reviewed and a recommendation based on the available literature and our experience for the management of pink pulseless hand in supracondylar fracture humerus is presented.
Mechanism of vascular injury
The mechanism of injury to the neurovascular structures following supracondylar fracture of the humerus has been described in great detail by Meyerding as early as 1936 [6]. He was the first to study the configuration of the fracture in detail and propose that in extension type supracondylar fractures, the injuring force carries the distal fragment posteriorly stripping the posterior periosteum. The sharp anterior fragment pierces the anterior periosteum and brachialis and injures the neurovascular bundle, which lies in close proximity anteriorly. The vascular insult could either be due to compression from the fragment, spasm or thrombosis or rarely complete arterial transection. Most times the absence of pulse might just be due to the compression of grossly displaced fragments. A gentle closed reduction would relieve the compression and artery becomes pulsatile again. Louahem et al. [7 described 26 patients with a pink pulseless hand in a series of 210 patients with severely displaced supracondylar fractures. In 21 cases, the pulses returned immediately after closed reduction of the fracture.
Collateral circulation
The exuberant collateral circulation around the elbow has been credited with maintaining the vascularity of the limb in patients managed without vascular exploration [8]. The radial recurrent artery arises distal to the elbow and anastomoses with the radial collateral branch of the profunda brachii. The superior ulnar collateral artery is the other main descending collateral. It arises from the brachial artery, a little below the middle of the arm and anastomoses with the posterior ulnar recurrent and inferior ulnar collateral arteries [8].
What is pink pulseless hand?
There is variable use of this terminology in the literature. Some authors use this terminology to label those supracondylar fractures presenting without a pulse with a well perfused hand. While there is no controversy regarding the management of these fractures, more than 50% of these pink pulseless limbs would turn pulsatile just after closed reduction. The limb appearing pink and perfused on presentation mainly depends on the time duration since injury, as it needs some time for the collateral circulation to be established. None of the authors had looked into the time since injury and its correlation to perfusion status at presentation. Ideally, a pink pulseless limb is one that remains pink and well perfused without a palpable pulse following closed reduction and pinning of a pulseless supracondylar fracture [2]. These are the ones that pose management controversy as to whether it needs urgent exploration for the vessel or a closed monitoring for the vascular status and just observation. Though there is some evidence in the literature supporting immediate exploration, more recent evidence seems to be in favour of in-patient observation and close monitoring [3].
Role of Doppler
There has been increased interest in the role of colour Doppler in the process of evaluation and decision making for pink pulseless hands. White et al has recommended the use of colour Doppler to assess the severity of arterial injury following closed reduction and pinning to decide on further management. A colour Doppler evaluation of the brachial artery would help to differentiate between spasm, thrombosis and complete transection. It is important to remember the fact that there is no question of brachial artery injury in this scenario and the real issue is about the adequacy of the collateral circulation to maintain the viability and function of hand. Doppler evaluation of the brachial artery might infact increase the number of explorations of the artery. Valentini et al has reported the use of color-coded duplex scanning (CCDS) and ultrasound velocimetry (UV) of the hand as an additional tool for evaluation in all their patients with pink pulseless hands [9]. In their series, all seven patients with pink pulseless hand were found to have brachial artery injury by Doppler and all of them were treated by arterial repair. But, there are no clear guidelines on severity of arterial injuries on colour dopper and their management. Using Doppler to assess the radial artery in a pink pulseless hand helps to assess the adequacy of the collateral circulation. Weller et al [10] in their series of 54 pulseless supracondylar humerus fractures have documented that 26 patients regained the pulse after closed reduction, 20 remained pulseless after closed reduction but radial artery Doppler signals were picking up and 4 others had absent pulse as well as Doppler signals. All four were taken up immediate surgical exploration and found to have arterial injury requiring repair. All 20 patients who had pulse detected by Doppler but had no palpable radial pulse were observed. One of the 20 developed late ischaemia after nine hours and was taken up for surgical exploration. Shah et al have included triphasic radial artery doppler signal in their algorithm for decision making in pink pulseless limbs and recommends immediate surgical exploration for patients who do not have triphasic radial artery doppler signals.
Proponents for Immediate Exploration
White et al [11] after a systematic analysis of pink pulseless supracondylar fractures have concluded that there is significant arterial injury in 70% of patients and thus vascular exploration may limit the chances of late complications in these patients. They have also stated that with reported patency rates of more than 90% it is worthwhile considering exploration and arterial repair in these patients. Korompilias et al. [7] reported on five patients with a pink pulseless hand and recommended vascular exploration for the restoration of brachial artery patency, even in the presence of a viable well-perfused hand after an attempt at closed reduction. Copley et al [13] in their series of 17 patients with pulseless supracondylar fractures had a return of pulse in 14 of them following closed reduction. All the three patients were taken up for exploration and 2 of the fourteen patients who developed loss of pulse over the next 24 hours were also explored. They recommend immediate exploration if pulse is absent after closed reduction as a measure towards prevention of late complications. Blakey et al. found that twenty three of twenty-six patients with a pink, pulseless hand following initial management had some evidence of ischemic contracture, and they advocated for urgent exploration when the pulse does not immediately return after closed reduction [14]. Mangat et al [15] reported on the predictive value of co-existing median or anterior interiosseous nerve injury after studying a series of patients with nerve injury who underwent exploration. A significant relationship was found between preoperative median and anterior interosseous nerve deficits and vascular entrapment and tethering of the nerve at the fracture site. The authors recommended early exploration for patients with a Gartland type-III supracondylar fracture when they have coexisting anterior interosseous or median nerve palsy as the benefits of exploration outweigh the disadvantages. In a recent study by Scannell et al [17], the authors have tried to correlate the presence of median or anterior interosseous nerve with patency of brachial artery at long term follow-up in 20 twenty patients. In their series, median nerve palsy had good prediction of brachial artery occlusion while anterior interosseous nerve palsy did not predict brachial artery occlusion.
Proponents for Observation
Many authors are in favour of observation and close monitoring of the vascular status for pink pulseless hands. In contrast to the general belief that the literature in vascular surgery would be more in favour of arterial exploration, the recent papers in vascular surgery are recommending observation in case of pink pulseless hands [3]. Choi et al [18] presented the largest series of 33 patients with pink pulseless hands and concluded that in patients presenting with well perfused hand, fracture reduction and pinning alone would be sufficient treatment. Scannell et al [17] have reported the long term results of their series of 20 patients of pink pulseless hand that were treated by observation. All 20 had good functional outcome except one who had chondrolysis of the distal humerus. They also recommended long term follow-up of these patients for radiographic evidence of osteonecrosis as three of their 20 patients with pink pulseless hands developed avascular necrosis of the trochlea. Weller et al [10] in their analysis of 20 patients with pink pulseless hands have concluded that lack of palpable radial pulse is not an absolute indication for arterial exploration if Doppler signals and capillary refill is good suggesting a well perfused hand. Matuszewski [19] has published his follow-up results of pulseless supracondylar humerus fractures have concluded that children who, after satisfactory closed reduction, have a well-perfused hand but absent radial pulse do not necessarily require routine exploration of the brachial artery. Sabharwal et al [20], in their follow-up study patients with pulseless supracondylar fracture who were treated with arterial exploration and revascularisation found a high rate of asymptomatic reocclusion and residual stenosis and hence opined that collateral circulation would have been adequate to maintain a viable extremity. Garbuz et al [21] in 1996 presented the outcome of treatment of supracondylar fractures with absent radial pulse from the Hospital for Sick Children, Toronto. In their series of 22 patients, five had pink perfused pulseless hands who were managed by close observation and all had excellent functional outcomes. They concluded that absent pulse is not an absolute indication for exploration, provided the hand remains well perfused and compartment syndrome does not develop.
Is there a Consensus?
Though the literature is filled with publications on pink pulseless hand in supracondylar fractures, there still seems to be no consensus on the management of this condition. The AAOS guidelines [22] for the management of supracondylar fractures of humerus in children published in 2010 stated that ”We cannot recommend for or against open exploration of the antecubital fossa in patients with absent wrist pulses but with a perfused hand after reduction of displaced pediatric supracondylar humerus fractures” as there was no strong evidence supporting either observation or exploration. Five years down the line, the question still remains unanswered as far as evidence goes. But, what has changed over the years is that now we have more objective ways of assessing the perfusion rather than just relying on pink colour of the hand and capillary refill. The use of Doppler ultrasound and pulseoximeter signals to assess the perfusion of limb have come into vogue [23]. The presence of associated median nerve injury is more predictive of a significant arterial injury and hence these patients should be considered for exploration.
Hence in the present scenario, three factors needs to be considered in the decision making process of pink pulseless hand:
1.Presence of radial artery Doppler signals
2.Presence of good pulseoximeter waveforms and oxygen saturation >95%.
3.Intact Median Nerve function.
If all the three criteria are met, the recommendation is to observe the child closely for circulation and symptoms of compartment syndrome. If all three are absent, it is an indication of poor perfusion and it is an indication for arterial exploration. The combination of absence of radial artery Doppler signals and absence of pulse oximeter signals again indicates poor perfusion and favors exploration. There is no evidence to comment on other scenarios of either isolated median nerve palsy or isolated absence of radial artery Doppler signals or pulse oximeter signals and their combinations. There are no studies, which have documented all these factors for all their patients, and we are not sure whether a limb can have absent radial artery Doppler signals with good pulse oximeter waveforms. These would rather be hypothetical situations and if someone comes across such a situation in clinical practice, the best would be to individually assess the case and decide for exploration versus observation. However, considering the complications and the reported incidence of significant arterial injuries up to 70% in patients without a positive radial artery Doppler signal, it may be a safer option to consider exploration in these patients. The use of Doppler of the brachial artery to know the severity of the arterial injury and taking it as a sole factor for considering exploration is not justifiable, as the limb can still have good collateral circulation. Thus in conclusion both clinical and diagnostic methods have to be taken into account while making a balanced decision in terms on observation or surgical exploration of a pink pulseless hand [3,24].
References
1. Schoenecker PL, Delgado E, Rotman M, Sicard GA, Capelli AM. Pulseless arm in association with totally displaced supracondylar fracture. J Orthop Trauma 1996; 10:410–415.
2. Robb JE. The pink, pulseless hand after supracondylar fracture of the humerus in children. J Bone Joint Surg Br. 2009 Nov;91(11):1410-2.
3. Badkoobehi H, Choi PD, Bae DS, Skaggs DL. Management of the pulseless pediatric supracondylar humeral fracture. J Bone Joint Surg Am. 2015 Jun 3;97(11):937-43.
4. Korompilias AV, Lykissas MG, Mitsionis GI, Kontogeorgakos VA, Manoudis G, Beris AE (2009) Treatment of pink pulseless hand following supracondylar fractures of the humerus in children. Int Orthop 33(1):237–241.
5. Matuszewski Ł. Evaluation and management of pulseless pink/pale hand syndrome coexisting with supracondylar fractures of the humerus in children. Eur J Orthop Surg Traumatol. 2014 Dec;24(8):1401-6.
6. MEYERDING HW. Volkmann’s ischemic contracture associated with supracondylar fracture of humerus. Journal of the American Medical Association, 1936:106:1139-1144.
7. Louahem DM, Nebunescu A, Canavese F, Dimeglio A. Neurovascular complications and severe displacement in supracondylar humerus fractures in children: defensive or offensive
strategy? J Pediatr Orthop B 2006; 15(1):51–57
8. Ramesh P, Avadhani A, Shetty AP, Dheenadhayalan J, Rajasekaran S. Management of acute ‘pink pulseless’ hand in pediatric supracondylar fractures of the humerus. J Pediatr Orthop B. 2011 May;20(3):124-8.
9. Benedetti Valentini M, Farsetti P, Martinelli O, Laurito A, Ippolito E. The value of ultrasonic diagnosis in the management of vascular complications of supracondylar fractures of the humerus in children. Bone Joint J. 2013 May;95-B(5):694-8.
10. Weller A, Garg S, Larson AN, Fletcher ND, Schiller JR, Kwon M, Copley LA, Browne R, Ho CA. Management of the pediatric pulseless supracondylar humeral fracture: is vascular exploration necessary? J Bone Joint Surg Am. 2013 Nov 6;95(21):1906-12.
11. White L, Mehlman CT, Crawford AH. Perfused, pulseless, and puzzling: a systematic review of vascular injuries in pediatric supracondylar humerus fractures and results of a POSNA questionnaire. J Pediatr Orthop. 2010 Jun;30(4):328-35.
12. Korompilias AV, Lykissas MG, Mitsionis GI, Kontogeorgakos VA, Manoudis G, Beris AE. Treatment of pink pulseless hand following supracondylar fractures of the humerus in children. Int Orthop. 2009 Feb;33(1):237-41.
13. Copley LA, Dormans JP, Davidson RS. Vascular injuries and their sequelae in pediatric supracondylar humeral fractures: toward a goal of prevention. J Pediatr Orthop. 1996 Jan-Feb;16(1):99-103.
14. Blakey CM, Biant LC, Birch R. Ischaemia and the pink, pulseless hand complicating supracondylar fractures of the humerus in childhood: long-term follow-up. J Bone Joint Surg Br. 2009 Nov;91(11):1487-92.
15. Copley LA, Dormans JP, Davidson RS. Vascular injuries and their sequelae in pediatric supracondylar humeral fractures: toward a goal of prevention. J Pediatr Orthop. 1996 Jan-Feb;16(1):99-103.
16. Luria S, Sucar A, Eylon S, Pinchas-Mizrachi R, Berlatzky Y, Anner H, Liebergall M, Porat S. Vascular complications of supracondylar humeral fractures in children. J Pediatr Orthop B. 2007 Mar;16(2):133-43
17. Scannell BP, Jackson JB 3rd, Bray C, Roush TS, Brighton BK, Frick SL. The perfused, pulseless supracondylar humeral fracture: intermediate-term follow-up of vascular status and function. J Bone Joint Surg Am. 2013 Nov 6;95(21):1913-9.
18. Choi PD, Melikian R, Skaggs DL. Risk factors for vascular repair and compartment syndrome in the pulseless supracondylar humerus fracture in children. J Pediatr Orthop. 2010 Jan-Feb;30(1):50-6.
19. Matuszewski Ł. Evaluation and management of pulseless pink/pale hand syndrome coexisting with supracondylar fractures of the humerus in children. Eur J Orthop Surg Traumatol. 2014 Dec;24(8):1401-6.
20. Sabharwal S, Tredwell SJ, Beauchamp RD, Mackenzie WG, Jakubec DM, Cairns R, LeBlanc JG. Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop. 1997 May-Jun;17(3):303-10.
21. Garbuz DS, Leitch K, Wright JG. The treatment of supracondylar fractures in children with an absent radial pulse. J Pediatr Orthop. 1996 Sep-Oct;16(5):594-6.
22. The treatment of pediatric supracondylar humerus fractures. AAOS Clinical Practice Guidelines Unit v1.0_092311. Summary of Recommendations. available from
http://www.aaos.org/research/guidelines/SupracondylarFracture/SupConFullGuideline.pdf
23. Soh RC, Tawng DK, Mahadev A. Pulse oximetry for the diagnosis and prediction for surgical exploration in the pulseless perfused hand as a result of supracondylar fractures of the distal humerus. Clin Orthop Surg. 2013 Mar;5(1):74-81.
24. Shah AS, Waters PM, Bae DS. Treatment of the “pink pulseless hand” in pediatric supracondylar humerus fractures. J Hand Surg Am. 2013 Jul;38(7):1399-403 .
(Abstract) (Full Text HTML) (Download PDF)
Supracondylar Humerus Fractures in Children: Epidemiology and Changing Trends of Presentation
Vol 1 | Issue 1 | July-Sep 2015 | page:3-5 | Sandeep V Vaidya.
Authors : Sandeep V Vaidya[1,2,3*].
[1] Children’s Orthopaedic Clinic, Thane.
[2] B J Wadia Children’s Hospital, Parel Mumbai
[3] Jupiter Hospital, Thane, Maharashtra, India
Address of Correspondence
Dr Sandeep V Vaidya
Director, Children’s Orthopaedic Clinic, Thane. India.
Email: drsvvaidya@gmail.com
Abstract
Diseases show a tendency to vary according to changing socio-economic trends and fractures too have shown this tendency. Paediatric supracondylar humerus fractures are one of the most common fractures seen by paediatric orthopaedic surgeons. There are few notable trends that have been reported and few other that I have personally noted in my practice and in practice of my colleagues. This article put together the changes reported in literature and tries to combine it with clinically relevant practical situations. Special focus is on fracture presentation and on decision making in management.
Keywords: Supracondylar Humerus fracture, classification, management.
Introduction:
Supracondylar humerus fractures in children are commonly seen in day to day practice. In this section, we study the epidemiology and changing trends of these fractures with respect to incidence, patient profile, types, modes of injury, treatment trends and complications.
Incidence:
Supracondylar humerus fractures (SHF) comprise 17% of all pediatric fractures and are second in frequency to forearm fractures. According to an epidemiological study, the incidence of fracture supracondylar humerus is 308/100000 per year in the general population. It is also the commonest pediatric fracture around the elbow. One epidemiological study identified supracondylar fractures in 206 out of 355 elbow fractures (58%) [1]. Barr reported a higher incidence of supracondylar humerus fractures during the vacations [2].
Age and sex:
If age distribution is considered, in the 0 to 7 year age group, SHF is easily the commonest fracture seen (28%) [3]. The mean age at which fracture supracondylar humerus occurs is 5 to 8 years [1,2]. Wilkins proposed that when a child falls on extended upper extremity, the patients who demonstrate hyperextension (cubitus recurvatum) of the elbow are more predisposed to have supracondylar fractures. The children who do not have hyperextension of the elbow tend to sustain fractures of the radius and the ulna, usually at the distal portion. Since ligamentous laxity with elbow recurvatum is seen in younger children, this explains the higher incidence of supracondylar humerus fractures in younger children and higher incidence of radius ulna fractures in older children.
Recently, there seems be increase in incidence of SHF in lower age group(less than 2 years). Fractures occurring in these very young children may pose a diagnostic dilemma because in many of these cases, the fracture line is extremely low and on plain radiographs may mimic a fracture lateral condyle humerus due to the largely cartilaginous component of the distal fragment. In such cases, additional imaging like MRI or arthrogram may be needed to differentiate these low supracondylar fractures from the lateral condyle fractures (Fig. 1). Another peculiarity of the low supracondylar humerus fractures is that such fractures can be complicated by Avascular necrosis of the trochlea with subsequent later sequelae.
Figure 1: (Case Courtesy Dr Sandeep Patwardhan)1a: Elbow radiograph`of a 2 year old child with fall on outstretched hand. The fracture line is extremely distal and only a flake of metaphysis is seen.1b,c: The fracture was treated by closed reduction and K wire pinning .
In most of the earlier studies, the fracture occurred much more commonly in boys than in girls. However in most of the recent series, the frequencies in girls and boys seems to be equalizing. Some series have actually reported a higher incidence in girls than boys[1,2]. This changing sex distribution may be attributed to more active participation of girls in sports activities.
Mode of injury:
The cause of fracture supracondylar humerus is accidental fall while playing in most of the cases (60 to 80 %). Road traffic accidents account for 10 to 20% of SHF [2]. High velocity trauma can lead to fractures with metaphyseal comminution or in rare cases fractures with intercondylar extension.
Child abuse is an uncommon etiology of SHF[4]. However Strait and colleagues reported supracondylar fractures from abuse in three of 10 abused children under the age of 3, and cautioned that SHF should not be assumed to have non-abusive causes without careful consideration [5].
Types:
Extension type is the commonest type, flexion type is seen in 1 to 3% cases [6]. The patients in the flexion-type group (mean age, 7.5 years) are significantly older than those in the extension-type group (mean age, 5.8 years). The fractures in flexion-type group are also more probable to require open reduction (31%) than those in the extension-type group (10%). The flexion-type group had a significantly increased incidence rate of ulnar nerve symptoms (19% vs 3% in the extension-type group) and need for ulnar nerve decompression [7].
Gartland classification is the commonest classification system used to grade supracondylar humerus fracture. Grade 1 fractures are the commonest, followed by Grade 2 and then Grade 3 [1,2].
In addition to these 3 types, Leitch et al described a type 4 fracture with multidirectional instability (unstable in both flexion and extension). This fracture type was noted in 9 out of 297 displaced fractures. These fractures are associated with high velocity trauma, the periosteal sleeve is completely torn and special manoeuvres are needed for closed reduction- pinning [8].
In extension type fractures the distal fragment may be displaced posteromedially or posterolaterally. Posteromedial displacement is commoner and seen in approximately 75% cases in most series. Posteromedial displacement of the distal fragment places the radial nerve at risk, whereas in fractures with posterolateral displacement the brachial artery and median nerve are at risk [9]. Bahk et al additionally classified extension type supracondylar fractures based on orientation of the fracture line in coronal as well as sagittal planes. In coronal plane, transverse fractures were the commonest (49%) followed by lateral oblique fractures (44%). Medial oblique (4%) and high transverse fractures (3%) were less common. Whereas transverse and lateral oblique fractures are amenable to lateral only pinning, the medial oblique and transverse fractures need to be fixed with medial-lateral cross pins [10].
High SHF are also being increasingly reported recently. Sen et al reported an incidence of high metaphyseal- diaphyseal supracondylar humerus fractures in 6 out of 182 fractures [11].
Treatment:
Blount in 1955 had cautioned against operative treatment in SHF citing the high incidence of complications following operative treatment [12]. However with significant advances in operative techniques and intraoperative imaging, operative treatment with Closed Reduction Percutaneous Pinning (CRPP) is easily the treatment of choice for displaced supracondylar humerus fractures [13]. Approximately 40% of SHF are treated operatively making it the commonest pediatric fracture to undergo operative treatment [2]. Cheng et al in an epidemiological study of 6493 fractures reported that the closed-reduction and percutaneous pinning rates for supracondylar humerus fractures increased 4.3 to 40% over a 10 year period from 1985 to 1995. The changes in treatment pattern were also accompanied by a corresponding decrease in the open-reduction rate and hospital stay periods from <10% to 38% of patients being discharged within 1 day of admission in the 10-year period [3].
The incidence of operative treatment is 0% in Grade 1 fractures, almost 50% for Grade 2 fractures, 100% for Grade 3 fractures and 100% for flexion type fractures. The incidence of open reduction is highest in flexion type fractures (50%) [2]. In an epidemiological study, out of 3235 children with displaced SHF treated operatively at a tertiary care children’s hospital at Toronto, 78.7% underwent operative treatment in the form of Closed Reduction Percutaneous Pinning (CRPP) whereas the remainder 21.8% underwent Open Reduction Internal Fixation (OR). There was a significant difference in the delay to surgery between the CRPP and OR groups [14]. In developed countries, there is a trend for more number of SHF are being treated by pediatric orthopaedic subspecialists. In New England, only 37% of SHF were treated by Pediatric Orthopaedic surgeons in 1991, this number rose to 68% in 1999. Kasser et al reported that in fractures treated by pediatric orthopaedic surgeons the length of hospitalization was lesser (1.4 ± 0.4 days) than for fractures treated by general orthopaedic surgeons (2.2 ± 0.6 days) [15]
Pin configurations, changing trends:
Pin configurations used by surgeons have shown a changing trend over the past decade. Several biomechanical studies published before 2005 revealed that crossed medial- lateral pin configurations are biomechanically stronger than lateral only pin configurations. Hence crossed medial- lateral pinning was preferred. However a major danger of the medial pin was iatrogenic ulnar nerve injury. Incidence of iatrogenic ulnar nerve injury with crossed medial- lateral pinning in various series has ranged from 0% to 6% [16,17]. Lyons et al reported iatrogenic ulnar nerve palsy in 19 out of 375 crossed medial- lateral pinning. 15 out of these 19 palsies recovered within 4 months after medial pin removal. However 4 palsies failed to recover, underwent ulnar nerve exploration and neurolysis [17]. A systematic pooled analysis of 32 trials comprising 2639 children suggests that there is an iatrogenic ulnar nerve injury for every 28 patients treated with the crossed pinning compared with the lateral pinning [16].
An inherent fallacy of the early biomechanical studies was that these studies were based on in-vitro findings wherein loads applied to create displacement were significantly higher than those which would be applied in-vivo wherein the fixation would be additionally supplemented with plaster slab application. Lee et al in their series of 61 consecutive lateral only pinning reported a zero incidence of loss of reduction as well as iatrogenic ulnar nerve palsy [18]. A randomized controlled study published in 2007 concluded that lateral entry only pinning did not result in increase incidence of loss of reduction as compared to crossed medial-lateral pinning [19]. A survey involving eight surgeons conducted in 2012 confirmed that this RCT had a significant influence on the surgeons’ practice. Five out of eight surgeons individually had a statistically significant change in their practice pattern for pin configuration. Except for certain selected fracture patterns, lateral only pinning is being increasingly used as the standard pin configuration for supracondylar humerus fractures [20].
Complications:
Complications of fracture supracondylar humerus include compartment syndrome, vascular injury, nerve injury (fracture related or iatrogenic) and malunion with cubitus varus deformity. The incidence of compartment syndrome is approximately 0.1% to 0.3% of all supracondylar humerus fractures [21]. Ipsilateral forearm fracture significantly increases risk of compartment syndrome [22]. In a study, the incidence of compartment syndrome was — % in fractures reduced and fixed within – hours of injury as compared to — % in fractures fixed after a delay of – hours.
The incidence of vascular injuries is approximately 20% and majority are associated with Grade 3 fractures [1, 23, 2]. Fractures with posterolateral displacement are more at risk for vascular injuries (approximately 65%) than fractures with posteromedial displacement (approximately 53%) [23]. If the hand is well perfused but pulseless, the great majority of the time fracture reduction is sufficient treatment. In contrast, patients presenting with a pulseless and poorly perfused hand have a nearly 50% chance of requiring vascular surgery and nearly 25% chance of developing a compartment syndrome [24, 25].
Nerve injuries are seen in approximately 4% fractures and majority are associated with Grade 3 fractures [1,2]. Overall, the most commonly injured nerve is median nerve (50%) followed by radial nerve (28%) followed by ulnar nerve (22%). The pattern of displacement is the most important risk factor in nerve injury. In fractures with median nerve palsy, posterolateral displacement is seen in 87% cases. In cases with radial nerve palsy, posteromdeial displacement Is seen in almost all cases [23] In flexion type, ulnar nerve is most commonly injured [7].
References
1. Houshian S, Mehdi B, Larsen MS. The epidemiology of elbow fracture in children: analysis of 355 fractures, with special reference to supracondylar humerus fractures. J Orthop Sci 2001;6(4):312-5
2. Barr LV. Pediatric supracondylar humeral fractures: epidemiology, mechanisms and incidence during school holidays. J Child Orthop. 2014; 8:167–170
3. Cheng, Jack CY, Ng, BKW, Ying, S. Y, Phil P. A 10-Year Study of the Changes in the Pattern and Treatment of 6,493 Fractures. 19(3), May/June 1999, pp 344-350
4. Kemp AM, Dunstan F, Harrison S, Morris S, Mann M, Rolfe K, Datta S, Thomas DP, Sibert JR, Maguire S. Patterns of skeletal fractures in child abuse: systematic review. BMJ 2008; 337:a1518
5. Strait RT, Siegel RM, Shapiro RA. Humeral fractures without obvious etiologies in children less than 3 years of age: when is it abuse? Pediatrics. 1995 Oct;96(4 Pt 1):667-71
6. Cheng JC, Lam TP, Maffulli N. Epidemiological features of supracondylar fractures of the humerus in Chinese children. J Pediatr Orthop B 2001;10(1):63-67
7. Mahan SD, May CD, Kocher MS. Operative Management of Displaced Flexion Supracondylar Humerus Fractures in Children. J Pediatr Orthop 2007;27:551-556
8. Leitch KK, Kay RM, Femino JD, Tolo VT, Storer SK, Skaggs DL. Treatment of multidirectionally unstable supracondylar humeral fractures in children. A modified Gartland type-IV fracture. J Bone Joint Surg Am. 2006 May;88(5):980-5.
9. Skaggs DL, Flynn JM. (2010) In Rockwood and Wilkins’ Fractures in Children. Philadelphia. Lippincott Williams and Wilkins. 514-515
10. Bahk MS, Srikumaran U, Ain MC, Erkula G, Leet AI, Sargent MC, Sponseller PD. Patterns of Pediatric Supracondylar Humerus Fractures. J Pediatr Orthop 2008;28:493-499.
11. Sen RK, Tripathy SK, Kumar A, Agarwal A, Aggarwal S, Dhatt S. Metaphyseo-diaphyseal junction fracture of distal humerus in children. J Pediatr Orthop B 2012, 21:109–114
12. Blount WP. Fractures in Children. Baltimore: Williams and Wilkins, 1955
13. France J, Strong M. Deformity and function in supracondylar fractures of the humerus in children variously treated by closed reduction and splinting, traction and percutaneous pinning. J Pediatr Orthop. 1992:12(4): 494-498
14. Khoshbin A, Leroux T, Wasserstein D, Wolfstadt J, Law PW, Mahomed N, Wright JG. The epidemiology of paediatric supracondylar fracture fixation: A population-based study. Injury. 2014; 45: 701–708Khoshbin A, Leroux T, Wasserstein D, Wolfstadt J, Law PW, Mahomed N, Wright JG. The epidemiology of paediatric supracondylar fracture fixation: A population-based study. Injury. 2014; 45: 701–708
15. Kasser JR. Location of treatment of supracondylar fractures of the humerus in children. Clin Orthop Relat Res. 2005 May;(434):110-3
16. Slobogean BL, Jackman H, Tennant S, Slobogean GP, Mulpuri K. Iatrogenic ulnar nerve injury after the surgical treatment of displaced supracondylar fractures of the humerus: number needed to harm, a systematic review. J Pediatr Orthop 2010;30(5):430-6
17. Lyons, James P. M.D.; Ashley, Edwin M.D.; Hoffer, M. Mark M.D. Ulnar Nerve Palsies After Percutaneous Cross-Pinning of Supracondylar Fractures in Children’s Elbows. J Pediatr Orthop. 1998:18, 43-45
18. Lee YH, Lee SK, Kim BS, Chung MS, Baek GH, Gong HS, Lee JK. Three Lateral Divergent or Parallel Pin Fixations for the Treatment of Displaced Supracondylar Humerus Fractures in Children. J Pediatr Orthop 2008;28:417-422
19. Kocher MS1, Kasser JR, Waters PM, Bae D, Snyder BD, Hresko MT, Hedequist D, Karlin L, Kim YJ, Murray MM, Millis MB, Emans JB, Dichtel L, Matheney T, Lee BM. Lateral entry compared with medial and lateral entry pin fixation for completely displaced supracondylar humeral fractures in children. A randomized clinical trial. J Bone Joint Surg 2007;89(4):706-12
20. Mahan ST, Osborn E, Bae DS, Waters PM, Kasser JR, Kocher MS, Snyder BD, Hresko MT. Changing Practice Patterns: The Impact of a Randomized Clinical Trial on Surgeons Preference for Treatment of Type 3 Supracondylar Humerus Fractures. J Pediatr Orthop 2012;32:340–345
21. Battaglia TC, Armstrong DG, Schwend RM. Factors affecting forearm compartment pressures in children with supracondylar fracture of the humerus. J Pediatr Orthop. 2002; 22(4): 431-439
22. Blackmore LC, Cooperman DR, Thompson GH. Compartment syndrome in ipsilateral humerus and forearm fractures in children. Clin Orthop and Relat Res. 2000; 376: 32-38
23. Campbell CC, Waters PM, Emams JB, Kasser JR, Millis MB. Neurovascular injury and displacement in type 3 supracondylar humerus fractures. J Pediatr Orthop. 1995;15(1):47-52
24. Choi PD, Melikian R. Skaggs DL. Risk Factors for vascular repair and compartment syndrome in the pulseless supracondylar humerus fracture in children. J Pediatr Orthop 2010;30:50-56 .
Epidemiology and Changing Trends of Presentation. International Journal of Paediatric Orthopaedics July-Sep 2015;1(1):3-5.
(Abstract) (Full Text HTML) (Download PDF)
Guest Editorial – Dr Peter Waters
Vol 1 | Issue 1 | July – Sep 2015 | page: 1 | Peter M Waters.
Authors: Dr. Peter M Waters.
M.D.Orthopedic Surgeon-In-Chief at Boston Children’s Hospital and
the John E. Hall Professor of Orthopedic Surgery at
Harvard Medical School. He is Current President of Pediatric Orthopaedic Society of North America (POSNA)
Guest Editorial
I am honored to write the editorial for the supracondylar humerus fractures in children symposium in the inaugural International Journal of Paediatric Orthopaedics. The manuscripts contained herein cover all the important issues in the care of the child with these potentially devastating injuries. Starting with epidemiology and classification systems, the authors address the importance of common language. This is imperative in order to make appropriate care decisions for each patient and to evaluate results among academic medical centers.
The indications for closed reduction alone, closed reduction and pinning versus open reduction fixation, is critical. So too, is the execution of any and all of these procedures. Supracondylar humerus fractures have the highest risk of complications of any pediatric fracture and proper application of surgical care in a safe, careful way lessens the risk of malunion, loss of motion, function, and need for further surgery. In brief, closed reduction, stable pinning, (usually now with 2-3 lateral entry pins) is the present standard of care for almost all displaced fractures that are not open or do not have neurovascular compromise.
The manuscript on the pink pulseless hand addresses the lack of consensus and the high variation of care in our highest risk patients for Volkman’s ischemic contracture, a disastrous result. . The patients with a pale pulseless hand are in some respects the most straightforward. Emergent exploration, decompression and if needed, reconstruction of the brachial artery at the site of injury is required. The pink, pulseless patient is harder to assess which patient will do well with observation versus which patient is on the way to compartment syndrome if we do not intervene. Clearly the presence of a median neuropathy increases the risk to the patient. If observation is chosen, it needs to be prolonged and the surgeon needs to ready to surgically intervene if the patient starts to deteriorate. It can be argued therefore, that safe exploration of the neurovascular bundle during fracture care of the pink pulseless hand is indicated. Advanced technology may help us better discriminate these patients in the future. The pink pulseless hand is not a zero risk situation and requires a high attention to detail to prevent a disaster.
The last portion of this iJPO symposium addresses complications and their treatment. Ideally we will get so skilled in our assessment and care of these children that we lessen the complications of injury and intervention. But problems do occur, and knowing how to properly care for them in a timely fashion (or refer to someone who can) is required.
Finally, the need to continue to learn and get better is addressed. Critically important for all of us and our patients. Our job is to get better generation by generation. I congratulate this team of surgeons on their contribution to the literature, our learning and hopefully better care of our patients.
Peter M. Waters MD.
(Abstract) (Full Text HTML) (Download PDF)
Growth Modulation in Children for Angular Deformity Correction around knee – Use of Eight Plate
Vol 1 | Issue 1 | July-Sep 2015 | page: 33-37 | Sandeep Patwardhan, Kunal Shah, Ashok K Shyam, Parag Sancheti.
Authors : Sandeep Patwardhan[1], Kunal Shah[1], Ashok K Shyam[1], Parag Sancheti[1].
[1] Sancheti Institute for Orthopaedics and Rehabilitation 16, Shivajinagar, Pune, India.
Address of Correspondence
Dr. Kunal Shah
Sancheti Institute for orthopaedics and Rehabilitation
16, Shivajinagar, Pune, India.
Email-orthokunal@yahoo.com
Abstract
Background: Angular deformities around the knee joint in skeletally immature children are treated with methods of reversible hemiepiphysiodesis like staples, transphyseal screw and eight plate. Hemiepiphysiodesis using Eight plate has showed good results with advantage being faster correction, less complications and can be used in younger age.
Methods: The aim of this retrospective study is show the efficacy of eight plate application and its complication rate. Nineteen patients (37 physes) (unilateral: 3; bilateral: 16) with angular deformity were treated with eightplate application. Seven with pathological physes and twelve with idiopathic physes. Outcome assessment was done clinically with calculation of intermalleolar /intercondylar distance and radiologicaaly with mechanical and anatomical axis. Correction achieved was considered when anatomical/mechanical axis were within normal limits and intermalleolar/intercondylar distance was less than 5 cm.
Results: The average age of intervention was 7.4±2.96 years (range 2.4 -11.2years). Rate of correction of IMD/ICD was 1.14 cm per month. Rate of correction of mechanical axis was 0.76 o per month. Rate of correction of anatomical axis was 1.04o per month. The average duration of eight plate removal 12.4 months (range 7-24 months).There were two complications one patient with screw backout and other with overcorrection.
Conclusion: Reversible hemiepiphysiodesis using eight plate is and effective method with minimal complications and faster rates of correction. Idiopathic physes show faster rates of correction than pathological physes. Physeal growth arrest is not seen with eight plate application. Larger data and long term follow up is required to assess the rebound deformity after eight plate removal.
Keywords: Reversible, hemiepiphysiodesis, angular deformity, eight plate.
Introduction
Pathological angular deformities of knee are common childhood deformities. Majority of them are idiopathic while others are due to some local or systemic cause [1].They present with cosmetic deformity, mild discomfort, gait disturbance, joint instability and limitation of activities or symptoms of causative disease. More importantly they predispose to early arthritic changes in the knee joint and secondary changes in hip and ankle joint [2, 3].Therefore it is important to identify them early and treat accordingly. Treatment depends mainly on cause of disease, age of child and amount of deformity. Corrective osteotomies once considered gold standard[3], are no longer advised in skeletally immature child, unless acute correction is required[4] or deformity is severe (>30o)[1]. Distraction osteogenesis using external fixator was used for gradual growth arrest, but it had several disadvantages like poor compliance, pin tract infections and longer time required to achieve correction [1].
Epiphysiodesis has emerged as the treatment of choice for angular deformity correction in skeletally immature patient with mild to moderate deformity[1,5]. Historically many methods for permanent and temporary epiphysiodesis were described [1]. Permanent methods depended on accurate timing of intervention to prevent overcorrection or under correction[5]. But none of the current methods of determining bone age are reliable [6, 7].Therefore reversible methods of epiphysiodesis have become the mainstay of treatment. It involves mainly staples, transphyseal screws and recently eight-plate has been used. Hemiepiphysiodesis with staples pose problems like migration, breakage and bending of implant, physeal growth arrest and rebound deformity[8].Transphyseal screws have shown fewer complications with implant and rebound phenomenon is less as compared to staples[5].However its reversibility is doubted by many as it cross the Physis[9,10]. Use of eight plate has shown promising results with fewer complications, faster correction and reversible growth [11, 12] yet literature is still sparse on use of this device. The purpose of this prospective study is to show the efficacy of hemiepiphysiodesis using eight-plate in correction of angular deformities around knee.
Material and Method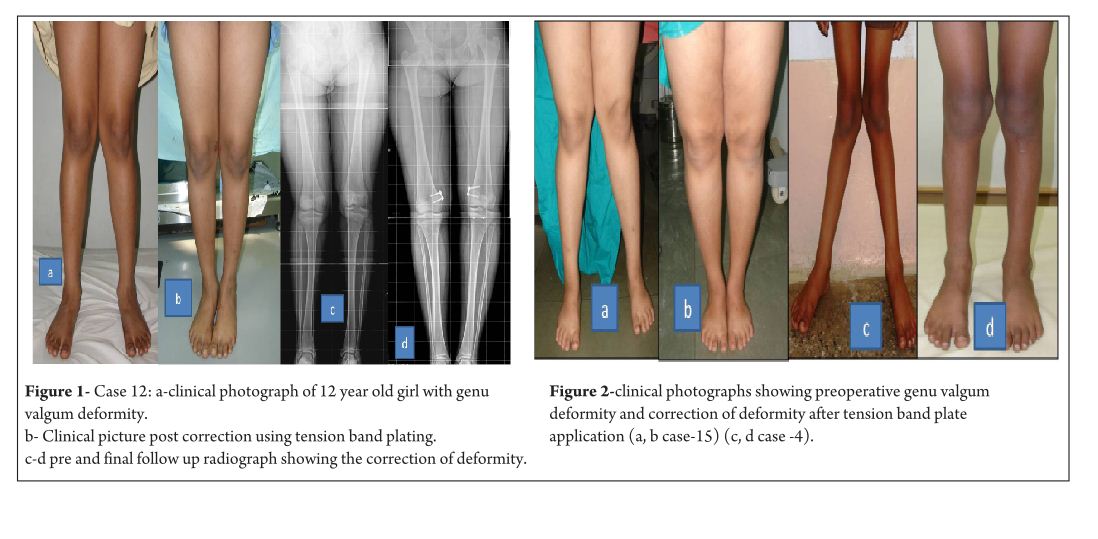
This is a retrospective study of 19 patients (37physes, 16 bilateral and 3 unilateral) with symptomatic angular deformity treated with 8 plate application. Out of the 19 patients there were 9 boys and 10 girls. Cause of angular deformity was rickets in 4, Down’s syndrome in 1, post septic in 1, skeletal dysplasia in 1 and idiopathic in 12. Genu varum was seen in 5 patients (8 physes) and genu valgum was seen in 14patients (29 physes).17 patients had 8 plate application in distal femoral physis, 1 patient had in proximal tibia and 1 patient had in both femur and tibia. Plates were applied in both tibia and femur to achieve faster rate of correction [11]. Surgical treatment was given to patients who were symptomatic or asymptomatic patients with age more than 4 years, with intermalleolar/intercondylar distance (IMD/ICD) more than 10 cm and/or mechanical axis more than 3° (valgum/varum). Contraindications to surgery included limbs with physiologic deformity, physeal arrest and maturity. Physiologic deformities were defined as genu varum in less than 2 years and genu valgum quantified by tibio-femoral angle less than 8° or IMD of less than 8 cm in age less than 4 years[14]. Physeal bar was defined as bony connection across physis, potentially affecting physeal growth [15]. The upper limit of age for surgical correction was at least one year of growth remaining [7, 9] as assessed on carpal age. In patient nearing skeletal maturity, hand film was taken to quantify amount of growth remaining. Standing lower limb scanogram with patella facing anteriorly [16] was taken preoperatively and at final follow up to look for mechanical axis and anatomical axis. Radiographically, mechanical axis of lower limb was measured as angle between mechanical axis of femur (centre of femoral head to centre of knee joint) and mechanical axis of tibia (centre of knee joint to centre of ankle mortise).The centre of knee joint was used to determine the mechanical axis [9]. The normal mechanical axis was considered as 0±3°[13]. With radiolucency of the physis it was difficult to define the centre of the knee joint and in such cases the centre of the distal physis of femur and proximal physis of tibia were considered in measurement. Tibiofemoral angle was measured as angle between long axis of femur and long axis of tibia. Normal was considered as 6° [16].
Clinically, intermalleolar and intercondylar distance were measured with patient in standing position with both patella facing forwards and medial malleolus/medial condyles just touching each other both preoperatively and at final follow up. Preoperative data was collected from the patient’s hospital records and from the surgeons own database. All patients with rickets were treated with appropriate medical management. Correction was considered when mechanical axis/anatomical axis were corrected and IMD/ICD was less than 5cm.
Surgical technique
With patient in supine position, tourniquet was applied to achieve haemostasis. Centre of Physis was marked using k wire under fluoroscopy guidance. Incision is taken and dissection done to reach the periosteum taking care that the periosteum is not breached and perichondrial blood supply is maintained. Plate inserted over the K wire and position confirmed under image intensifier, cannulated screws inserted parallel to Physis. Screw position checked under image intensifier in both antero-posterior and lateral view. Closure done and dressing applied. Postoperatively no immobilisation was required and patients were mobilised full weight bearing as tolerated from post op day 1. No walking support was required. Patients were followed up prospectively at every 3 month and knee radiographs were taken antero-posterior and lateral view to look for screw divergence and clinically IMD/ICD was measured.
Results
The average age of intervention was 7.4±2.96 years (range 2.4 -11.2years).The mean values of mechanical axis, tibiofemoral axis, IMD/ICD and duration of correction were calculated excluding the patient with overcorrection [case no 19] to avoid wide deviation from mean values. The mean preoperative IMD/ICD was 15.8cm ± 3.96 (range 10 cm to 22 cm) .The mean correction 1.6cm ± (range 0cm to 4 cm). Rate of correction was 1.14 cm per month. The mean preoperative mechanical axis was 13.4o± 5 (range7o to 25o).The mean post operative mechanical axis was 3.9o ±2.44 (range 0o to 10o). Rate of correction was 0.76 o per month .The mean preoperative tibiofemoral angle was 18.7o ±5.1 (range 7o -28o). The mean post operative tibiofemoral angle was 5.8o ± 2.29 (range 0o -12o). Rate of correction was 1.04o per month .Rate of correction in idiopathic and pathological physis group are depicted in table 1 and 2).The average duration of eight plate removal was 12.4 months (range 7-24 months). It was 13.3 months in pathological group and 11.8 months in idiopathic group. Figure 1 shows clinical and radiological correction in terms of IMD/ICD, mechanical axis and tibiofemoral axis. One patient was excluded from the data, a case of pathological genu valgum because the physis became fused before correction was achieved .The patient was treated with corrective osteotomy. Thus, emphasizing on preoperative planning in terms of age of intervention and aetiology deformity. There were two complications; one patient had screw back out which was revised. Other patient had reversal of deformity from 24° valgus to 22° varus due to delayed follow up [case 19]. She was treated with removal of 8 plate and is currently under observation for spontaneous correction. None of the patient had limb length discrepancy except (case 12) had 3 cm femoral shortening. Clinical data and outcome assessment in idiopathic and pathological group are depicted in table 1 and table 2.
Discussion
Physeal growth in child depends on variety of factors like biomechanical, hormonal and genetic [17]. Growth modulation using eight-plate depends on biomechanical growth modification based on Hueter-volkmann principle. Sustained compression parallel to physis leads to growth retardation and subsequent correction of deformity [9]. Eight-plate functions as flexible device which produces sustained compression at physis. The compression is not constant as the screws diverge with correction and with maximum divergence the plate bends, hence also called as tension band plate [11]. Eight-plate serves as non rigid implant with lateralisation of fulcrum for deformity correction. Thus, leading to faster rates of correction [ 2, 8]. Staples and transphyseal screws are rigid implants with centralised fulcrum for deformity correction [13]. They produce constant compression at physis. Thus they take longer time for deformity correction [2, 8]. Staples and transphyseal screws are rigid implants and if a prolonged duration is required for correction of deformity, they may cause physeal arrest [17]. In contrast eight plates are relatively flexible implants as it allows for screw separation. This is one of the reasons for decreased incidence of physeal arrest and makes it safer to use in younger children when compared to staples. In our study, three patients below the age of 3 years were treated successfully without any complications [case no 2, 7 and 11]. Clinical assessment of growth modulation by using IMD/ICD is reported for studies using staples [18] but not in studies using eight-plate. Since IMD/ICD was the major criteria to define the indication for surgery in our series, we have used the same as the primary outcome measure. We believe that IMD/ICD is an important clinical measure as majority of our patient were asymptomatic with cosmetic deformity and follow up parent counselling was easier. However standard values for particular age and race vary [14, 19].There can also be high rate of inter observer discrepancy and this is one of the limitations of the study. Radiographic measurements are used as outcome measures in papers on growth modulation using eight-plate like tibio-femoral axis, mechanical axis, joint orientation angles, mechanical axis deviation , articular –diaphyseal etc[2,10,11,20]We have used two radiological outcome measures, the hip knee ankle mechanical axis and the tibio-femoral angle. In our study we found that tibiofemoral angle and mechanical axis improved significantly. Standard antero-posterior and lateral radiographs of knee joint are useful in follow ups to see the effect of epiphysiodesis as seen with screw divergence. Joint orientation angles were not used, as scanograms become distorted due to magnification and parallax leading to false values[6].Also in young children it is difficult to visualise the distal femur and proximal tibia epiphyseal contours to accurately mark these angles. Ballal et al [11] showed that mean rate of correction of tibiofemoral axis 0.7°/month for distal femur and 0.5°/month in proximal tibia. Burghardt et al [20] showed mechanical axis correction of 1.73mm/month. In our study mean rate of correction of mechanical axis was 0.76°/month and tibio-femoral axis was 1.04°/month.
Rate of correction is faster in children less than 10 years as shown in study by Ballal et al [11]. In our study, due to smaller sample size of patients more than 10 years of age we could not assess this in our series. We did compared the rate of correction between the idiopathic and pathological group with former showing faster correction (Table 3 and 4). This corroborated with findings of Boero et al.No difference in rate of correction was encountered in terms of gender and type of deformity in our series. In our study two complications occurred, one patient had a screw back out (figure 3a) at 4 month after insertion, which was treated with revision of screw. However the rate of deformity correction was consistent with other patients in idiopathic physis group. We believe that the reason for back out may be placement of screw near the posterior cortex. Similar complications of screw loosening were seen in studies by Burghardt (n=1) [20] and Stevens (n=1) [2]. Other complication of overcorrection of deformity (figure 3b) was seen in one patient because of delayed follow up. This is justified as principally the sustained compression at physis will produce dynamic changes. Ballal et al [11] encountered one case of both screw and plate migration which was revised, such complication didn’t occur in our series. Several series encounter rebound growth after plate removal [2, 11, 20], we have not seen rebound of deformity in our patient with longest follow up of 2 years after plate removal. Complications related to implant like migration, breakage, bending of implants etc seen with staples are less common with eight -plate. Most dreaded complication of physeal arrest is not reported in our and other series [2, 3, 7, 10, 11, 20]. The threaded screws are less likely to extrude, especially in cartilaginous physis seen in younger age [8]. Screws are placed extra-periosteal and perichondrial blood supply is not hampered, so the chances of physeal arrest while insertion and removal are very less. Our study has drawbacks of small sample size and retrospective study design. However it does gives important inferences in terms of ability of 8 plates to correct the deformity and more importantly with minimal complications. However larger sample comparative studies will be required to establish the superiority of this method compared to other methods. Each author certifies that he or she has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
References
1. Celestre PC, Bowen RE. Correction of angular deformities in children- Current Orthopaedic Practice. 2009;20(6):641-647.
2. Stevens PM. Guided growth for angular correction: a preliminary series using a tension band plate. J Pediatr Orthop. 2007 Apr-May; 27(3):253-9.
3. Wiemann JM 4th, Tryon C, Szalay EA. Physeal stapling versus 8-plate hemiepiphysiodesis for guided correction of angular deformity about the knee. J Pediatr Orthop. 2009 Jul-Aug; 29(5):481-5.
4. Cho TJ, Choi IH, Chung CY, Yoo WJ, Park MS, Lee DY. Hemiepiphyseal stapling for angular deformity correction around the knee joint in children with multiple epiphyseal dysplasia. J Pediatr Orthop. 2009 Jan-Feb; 29(1):52-6.
5. Ghanem I, Karam JA, Widmann RF. Surgical epiphysiodesis indications and techniques: update. Curr Opin Pediatr. 2011 Feb; 23(1):53-9.
6. Friend L, Widmann RF. Advances in management of limb length discrepancy and lower limb deformity. Curr Opin Pediatr. 2008 Feb; 20(1):46-51.
7. Burghardt RD, Herzenberg JE, Standard SC, Paley D. Temporary hemiepiphyseal arrest using a screw and plate device to treat knee and ankle deformities in children: a preliminary report. J Child Orthop. 2008 Jun; 2(3):187-97.
8. Eastwood DM, Sanghrajka AP. Guided growth: recent advances in a deep-rooted concept. J Bone Joint Surg Br. 2011 Jan; 93(1):12-8.
9. Stevens PM. Guided growth of the lower extremities. Current Orthopaedic Practice. March/April 2011; 22(2):142–149
10. Schroerlucke S, Bertrand S, Clapp J, Bundy J, Gregg FO. Failure of Orthofix eight-Plate for the treatment of Blount disease. J Pediatr Orthop. 2009 Jan-Feb; 29(1):57-60.
11. Ballal MS, Bruce CE, Nayagam S. Correcting genu varum and genu valgum in children by guided growth: temporary hemiepiphysiodesis using tension band plates. J Bone Joint Surg Br. 2010 Feb; 92(2):273-6.
12. Stevens PM, Klatt JB. Guided growth for pathological physes: radiographic improvement during realignment. J Pediatr Orthop. 2008 Sep; 28(6):632-9.
13. DeBrauwer V, Moens P. Temporary hemiepiphysiodesis for idiopathic genuavalga in adolescents: percutaneous transphyseal screws (PETS) versus stapling. J Pediatr Orthop. 2008 Jul-Aug; 28(5):549-54.
14. Heath CH, Staheli LT. Normal limits of knee angle in white children–genu varum and genu valgum. J Pediatr Orthop. Mar-Apr 1993.
15.Paterson HA Epiphyseal growth plate fracture. Springer, Berlin 2007.
16. Paley D. Principles of Deformity Correction. Berlin, Germany: Springer; 2002.
17. Frost HM, Schönau E. On longitudinal bone growth, short stature, and related matters: insights about cartilage physiology from the Utah paradigm. J Pediatr Endocrinol Metab. 2001 May; 14(5):481-96.
18. Courvoisier A, Eid A, Merloz P. Epiphyseal stapling of the proximal tibia for idiopathic genu valgum. J Child Orthop. 2009 Jun; 3(3):217-21.
19. Omololu B, Tella A, Ogunlade SO, Adeyemo AA, Adebisi A, Alonge TO, Salawu SA, Akinpelu AO. Normal values of knee angle, intercondylar and intermalleolar distances in Nigerian children. West Afr J Med. 2003 Dec; 22(4):301-4.
20. Burghardt RD, Herzenberg JE. Temporary hemiepiphysiodesis with the eight-Plate for angular deformities: mid-term results. J Orthop Sci. 2010 Sep; 15(5):699-704.
21. Boero S, Michelis MB, Riganti S. Use of the eight-Plate for angular correction of knee deformities due to idiopathic and pathologic physis: initiating treatment according to etiology-J Child Orthop 2011;5(3):209-216.
(Abstract) (Full Text HTML) (Download PDF)
Apophyseal Metaphyseal combination injury to Olecranon in a healthy Adolescent – A rare injury and review of literature
Vol 1 | Issue 1 | July-Sep 2015 | page:51-53 | Ganesh Singh Dharmshaktu, Anshuman Vijay Roy.
Authors : Ganesh Singh Dharmshaktu[1], Anshuman Vijay Roy[2].
[1] Department of Orthopaedics, Government Medical College, Haldwani , Uttarakhand.
[2] Department of Orthopaedics, Krishna Hospital and Research Centre, Haldwani , Uttarakhand.
Address of Correspondence
Dr. Ganesh Singh Dharmshaktu , Department of orthopaedics , Government Medical College , Haldwani ( Uttarakhand ) . PIN -263139. Email: drganeshortho@gmail.com
Abstract
Background: Apophyseal injuries of olecranon have limited number of case reports and series owing to its rarity. Pure apophyseal avulsions are very rare and so are apophyseal metaphyseal combination injuries. No guidelines exist for the uniformity of the treatment and various modalities have been tried in sporadic reports. A keen clinical observation is required to suspect the possibility of these injuries followed by good imaging confirmation. Concordance of associated disorders like osteogenesis imperfecta with such injuries underlines the importance of ruling out this clinical entity in such cases.
Keywords: Fracture, Apophysis, Olecranon, Injury. Tension band wiring.
Introduction
Upper extremity is common site of bony injuries in children with reported incidence of 65% to 75% in the literature. 7% to 9% of these injuries are elbow injuries.[1] Apophysis is a term usually applied to an epiphysis that is subjected to traction by muscle insertion and its physiological pull.[2] The injury to the region if displaced can cause serious morbidity and functional limitation and thus warrants appropriate treatment. Non operative management is limited to only undisplaced injuries while injuries with more than 3-5 mm. of displacement warrants open reduction followed by fixation with varying methods. Open reduction and compressive fixation has widely been tried successfully with various implants like screws, tension band wiring or resorbable sutures. There has not been significant growth related problem with compression forces as a result of internal fixation.[2]
Case Report
A 12 year old boy was presented to us with history of injury to his right elbow following fall from height two days back. He was taken to a local practitioner before coming to us with a make do splint of wooden sticks. There was swelling, pain and difficulty in using the affected limb. There was tenderness present and swelling more over the posterior aspect but no raised temperature and intact distal neurovascular status. There was no appreciable crepitus or frank abnormal mobility present and a proper elbow examination including range of motion status was limited by swelling and pain. The radiograph of the affected elbow showed an apophyseal-metaphyseal combination injury with displacement. The olecranon apophysis with a rim of metaphysis was avulsed. There was no associated injury present. There was neither any history of frequent or multiple bony injuries in the past related or remote to present condition nor presence of blue sclera or abnormal dentition. The parents of the boy were explained and advised operative intervention of the injury. Following an informed consent of parents in view of patient being minor and under aseptic precautions open reduction and internal fixation was planned and carried out.
Result
The open reduction and internal fixation was performed and secured with tension band wiring (TBW). The posterior approach was used to access the injury site, The avulsed part was provisionally reduced and held together with pointed clamps while TBW was carried out in standard manner using two parallel Kirschner’s wires and a wire loop in figure of eight fashion. The operation went uneventful and so was peri-operative period. The stitches were removed on tenth day and patient was advised supervised physiotherapy after two weeks. The follow up initially at three, six twelve weeks and then after three and six months were uncomplicated and the range of motion improved all this while. The final follow up at six months showed normal range of motion as compared to contra-lateral side. There was no problem with hardware in the follow up and those were removed subsequently after months.
Discussion
The type 3 injuries related to olecranon apophyses are complete fractures with type 3 (a) as pure avulsions and type 3(b) as apophyseal-metaphyseal combination injuries.[2] Type 3(b) injuries are commoner in older children while type 3(a) usually involves younger children. This pattern of injury has been likened to Salter-Harris type 2 injury.[3] Apophyseal injuries of olecranon are uncommon with limited reported incidents.[4] Most of these injuries have been associated with patients of osteogenesis imperfecta.[5] Osteognesis imperfecta cases ( like tarda form) show higher incidences for this injury.[6] Apart from the fact that olecranon apophyses fractures are reported in relation with 50% cases of osteogenesis imperfecta, there have been reportedly higher rates of complication such as refracture in them.[7] It has been advised that hardwares should be maintained even after union in cases of osteogenesis imperfect due to this risk.[5,7] The elbow has rich vascularity with extraosseus network as well as intraosseus one.[8,9] The undisplaced fractures are amenable to conservative treatment with plaster of paris slab or cast and fracture unite well if length, angulation and rotation is properly taken care of. The displaced fractures has been managed with tension band wiring in most instances with fair to excellent results.[3,7,10] Some authors have used trans- osseous suture fixation for the fractures with good results.[11] Use of absorbable wires as supplemental fixation have also been reported.[12] As most of these injuries occur in children near skeletal maturity, no significant growth related problem is seen as compressive fixation across physes. The presented case is an uncommon variant of apophyseal olecranon injury in a normal child managed satisfactorily with appropriate techniques.
References
1. Landin LA, Danielsson LG. Elbow fractures in children: an epidemiological analysis of 589 cases. Acta Orthop Scand 1986; 57:309.
2. Erickson M, Frick S. Fractures of the proximal radius and ulna.In Beaty JH, Kasser JR. editors. Rockwood and Wilkins Fractures in children 7th ed. Philadelphia: Lippincott Williams and Wilkins;2010: 427-431.
3. Granthan SA, Kiernan HA. Displaced olecranon fractures in children. J Trauma 1975;15197-204.
4. Carney JR, Fox D, Mazurek MT. Displaced apophyseal olecranon fracture in a healthy child. Mil Med. 2007;172(12):1225-7.
5. Zionts LE, Moon CN. Olecranon apophysis fractures in children with osteogenesis imperfecta revisited. J Pediatr Orthop.2002; 22(6):745-50.
6. Di Cesare PE, Sew-Hoy A, Krom W. Bilateral isolated olecranon fractures in an infant as presentation of osteogenesis imperfect. Orthopedics 1992; 15:741-743.
7. Gwynne-Jones DP. Displaced olecranon apophyseal fractures in children with osteogenesis imperfecta. J Pediatr Orthop. 2005; 25(2):154-7.
8. Wilson PD. Fractures and dislocations in the region of elbow. Surg Gynecol Obstet 1933;56:335-359.
9. Haraldsson S. The intraosseous vasculature of the distal end of humerus with special reference to capitellum. Acta Orthop Scand 1957;27:81-93.
10. Poland J. A Practical Treatise on Traumatic Separation of the Epiphyses. London; Smith, Elder & Co, 1898.
11. Rath NK, Carpenter EC, Thomas DP. Traumatic pediatric olecranon injury: a report of suture fixation and review of the literature. Pediatric emergency care 2011; 27(12):1167-9.
12. Gortzak Y,Mercado E, Atar D, et al. Pediatric olecranon fractures: open reduction and internal fixation with removable Kirschner wires and absorbable sutures. J Pediatr Orthop 2006;26:39-42 .
(Abstract) (Full Text HTML) (Download PDF)